
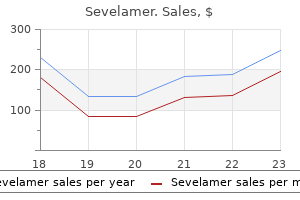
Sevelamer dosages: 800 mg, 400 mg
Sevelamer packs: 10 pills, 30 pills, 60 pills, 120 pills, 90 pills

Sevelamer 800 mg on-line
A main problem with liver resection in cirrhotic sufferers, even minor procedures, is postoperative decompensation, together with liver failure and ascites (see Chapters 76 and 103D). In explicit, we observed less postoperative ascites than previously experienced after open surgery. This was confirmed by a quantity of authors and in meta-analyses (Belli et al, 2009b; Morise et al, 2015; Sasaki et al, 2009). It seems that laparoscopy itself could supply some protection from postoperative decompensation. Reasons could include less fluid requirement, avoidance of long abdominal incisions with muscle division, higher collateral preservation, less manipulation, and less respiratory impairment. In our expertise, however, colorectal liver metastases have been much less amenable to a laparoscopic method. This is the outcomes of our referral base consisting mainly of bilobar or difficult-to-resect liver metastases. The noticed pattern has been toward a better proportion of benign disease being handled laparoscopically, because these pathologies are extra amenable to a minimally invasive strategy because of the next incentive in younger sufferers, and no margins are required. In this respect, bilobar disease, particularly in the case of colorectal liver metastases, is considered a contraindication to the laparoscopic method by most teams because of the risk of missing some lesions or performing an inadequate oncologic procedure (see Chapter 92). Case-control studies have demonstrated decrease morbidity (Belli et al, 2009b; Laurent et al, 2003; Sasaki et al, 2009), shorter size of hospitalization (Buell et al, 2008; Cai et al, 2008; Koffron et al, 2007; Topal et al, 2008), less operative blood loss (Bryant et al, 2009; Buell et al, 2008; Koffron et al, 2007; Lesurtel et al, 2003), reduced transfusion requirements (Buell et al 2008; Koffron et al, 2007; Topal et al, 2008), a decreased need for analgesia and faster return to oral consumption (Cai et al, 2008; 2009), and fewer postoperative adhesions (Belli et al, 2009a; Laurent et al, 2009). Studies have demonstrated decreased prices when accounting for shorter operative time and size of hospital stay (Buell et al, 2008; Koffron et al, 2007; Polignano et al, 2008). The mortality charges in these studies are no less than equivalent to those of enormous case sequence of open liver resections. Of 37 deaths, the cause of demise was attributed to bleeding, sepsis, or liver failure. Liverspecific issues accounted for 4% and included bile leaks, transient liver failure and ascites, and abdominal collections. The remaining 6% have been complications common to all operations, including however not restricted to hemorrhage, wound infection, hernia, bowel harm, intraabdominal fluid accumulation, and urinary or respiratory tract infections. As a consequence of decreased adhesions formed after an preliminary laparoscopic resection, reoperations similar to repeat hepatectomy and liver transplantation can usually be carried out more simply with much less blood loss, lowered transfusion requirements, and lowered operation time than after an preliminary open hepatectomy (Belli et al, 2009a; Bryant et al, 2009; Laurent et al, 2003, 2009). Barriers to the extensive acceptance of laparoscopic hepatic surgery-such as threat of gas embolism, violation of oncologic principles, and significant risk of bleeding-have not been obvious in the literature (Vigano et al, 2009b). In addition, research have constantly demonstrated that operative security and postoperative morbidity improve with expertise (Nguyen et al, 2009a). When evaluating our early and late groups, we discovered statistically significant reductions in operative time (from 210 to 150 minutes), blood loss (300 to 200 mL), conversion (16. Additional benefits embody better cosmesis and improved maintenance of the sensorimotor integrity of the abdominal wall. Despite these favorable outcomes, it could be very important acknowledge that these findings are from nonrandomized research, and that laparoscopic instances stay extremely chosen for his or her potential for achievement. It can be inferred from the colorectal and bariatric literature that these advantages are actual. As such, parenchyma-sparing procedures must be promoted in anticipation of repeat operative wants. The heart should have an enough backup provide of cameras, screens, insufflators, electrical surgical procedure turbines, cables, tubings, and laparoscopic instruments. A set of conventional instruments for open surgical procedure should be available in case of want for conversion. A versatile laparoscope is also helpful for better view, particularly in posterior areas of liver. Although it has not but been shown to improve outcomes, its supporters report enhanced high quality of vision and suturing, recognition of dissection aircraft, and liver parenchymal transection. A carbon dioxide insufflator to maintain a pneumoperitoneum of roughly 12 mm Hg is used. Some authors suggest quickly growing pneumoperitoneum, up to 15 mm Hg or greater in case of bleeding. This could help controlling venous bleeding but might enhance the danger of fuel embolism. Hand-assisted laparoscopy can be utilized for lesions in difficult-to-approach areas or as wanted to facilitate the process or acquiring hemostasis.
Purchase sevelamer 400 mg fast delivery
Distal pancreatectomy stays the mainstay of therapy of patients with major ductal disruption (Balasegaram & Lumpur, 1976; Heitsch et al, 1976). Pancreatic trauma continues to tax the judgment and operative abilities of skilled surgeons, at the identical time as subtle, minimally invasive strategies evolve. In addition, the complicated pancreatic anatomy dictates that the head and the body of the pancreas be managed operatively as two separate organs. The spleen has the closest anatomic relationship to the injured physique and tail of the pancreas. The pancreatic physique is usually approached by first mobilizing the spleen medially to Chapter 123 Pancreatic and duodenal accidents 1899 enter the anatomic aircraft behind the spleen and pancreas. The splenic artery and vein are then easily uncovered and controlled on the posterior floor of the gland; however, if essential, control of the splenic vessels could be achieved by mobilizing the physique of the gland alongside its superior and inferior aspects, without splenic mobilization. Based on this anatomic arrangement, trauma surgeons view the physique and tail of the pancreas as an organ with a single accessible vascular pedicle, much like the kidney or spleen. When necessary, the injured pancreatic physique may be easily resected by performing an en bloc distal pancreatectomy and splenectomy. The main concern in trauma is whether or not the principle pancreatic duct is broken, as a outcome of this will cause a persistent fistula with its related complications. Above it, just behind and beneath the gland, are the portal vein and superior mesenteric vessels. The uppermost layer consists of the gastroduodenal artery and pancreaticoduodenal arcades. For practical purposes, trauma to the pancreas ranges from superficial accidents that require only drainage (Kantharia et al, 2007) to ductal disruption that mandates a distal pancreatectomy. Low-grade injuries to the duodenum can be repaired the same as any other penetrating damage to the intestine; nevertheless, highgrade duodenal injuries, and especially those that mix duodenal and pancreatic trauma, require a different approach because of the excessive risk and unforgiving nature of a duodenal leak. This perspective on pancreatic anatomy types the basis for a detailed dialogue of the administration of pancreatic injuries in the forthcoming sections. Diagnosis of Pancreatic and Duodenal Trauma Hemodynamically secure sufferers with injuries to the pancreas and/or duodenum may exhibit solely refined indicators due to the retroperitoneal location of those organs. Patients with a historical past of acceleration/deceleration harm; forceful anterior compression of the abdomen, such as from kicks or handlebar accidents; and lower thoracic and upper lumbar vertebra fractures are at elevated risk. A "seat belt sign" across the higher and middle stomach ought to suggest the potential for critical intraabdominal injury (Bansal et al, 2009). However, the physical examination can be remarkably benign; abdominal pain and peritoneal indicators typically take days to develop. For all these reasons, a excessive index of suspicion is essential to keep away from lacking an damage (Wright & Stanski, 2000). Patients with elevated white blood cell depend, amylase, or lipase clearly require further investigation; sadly, many patients are seen with normal values. In reality, as many as 35% of patients with a pancreatic transection have normal amylase levels (Adamson et al, 2003; Jones, 1985; Sriussadaporn, 1994; Takishima et al, 1997). However, the process itself has the potential to trigger pancreatitis (Cotton et al, 2009; Silviera et al, 2009) and is usually indicated solely when prognosis of a lacerated duct will change the administration of the injury. Operative Management of Injuries to the Body and Tail of the Pancreas (See Chapter 66) the operative approach to injuries to the physique and tail of the pancreas is analogous for both blunt and penetrating accidents. Full exposure is achieved by both dividing the gastrocolic ligament or by freeing the larger omentum from the transverse colon, reflecting the abdomen up, and taking down any adhesions between the posterior wall of the abdomen and the retroperitoneum. Any area of harm, contusion, or hematoma is explored by opening the posterior peritoneum over the anterior facet of the pancreas, as a outcome of a superficial and seemingly harmless hematoma may disguise a deep laceration. Severe bleeding virtually by no means originates from the pancreas itself but quite from adjoining constructions. In assessing the physique and tail of the pancreas, the vital thing query that the surgeon should handle is whether or not a pancreatic duct injury is present (Bach & Frey, 1971; Bradley et al, 1998; Tyburski et al, 2001; Voeller et al, 1991). The integrity of the duct can be interrogated by intraoperative imaging, either by amputating the tail and cannulating the distal duct or by cannulating the gallbladder and injecting distinction into the common bile duct. The extra sensible possibility in the course of the night time is just to proceed with empiric distal pancreatectomy, each time a deep laceration is within the neighborhood of the main pancreatic duct, or a big hematoma is discovered in the center of the gland. An different choice for nonbleeding pancreatic accidents, notably within the face of multiple related accidents, is closed-suction drainage of the lesser sac.
Order genuine sevelamer
However, apomorphine has strong emetic effects, and an antiemetic such as trimethobenzamide have to be administered prophylactically, sometimes for 3 days, before initiating remedy with apomorphine. Antimuscarinics are helpful in some sufferers for controlling tremor and drooling and should have additive therapeutic results at any stage in the illness. They may be used for short-term monotherapy in tremorpredominant disease, however have little value for akinesia or impaired postural reflexes. Interventions that diminish nigrostriatal dopaminergic neurotransmission lower spontaneous normal motion and attenuate or get rid of choreiform movements. These brokers are additionally used to treat other hyperkinetic movement problems, together with tic disorders and tardive dyskinesia. Diminished dopaminergic transmission in the nigrostriatal system is liable for the attenuation of chorea. However, excessive blockade can diminish normal, spontaneous movement and lead to parkinsonism (slowness, rigidity, rest tremor). The atypical antipsychotics have been used to control chorea with varying levels of success. Selegiline is rapidly absorbed and metabolized to N-desmethylselegiline, amphetamine, and methamphetamine with half-lives of two, 18, and 20 hours, respectively. Rasagiline is also rapidly absorbed, but when taken with a meal containing excessive fat, absorption decreases substantially. Safinamide can also be quickly absorbed, with peak plasma levels reached at 2�4 hours and a half-life of roughly 22 hours. Safinamide is metabolized primarily by nonmicrosomal enzymes to inactive products. Ropinirole and pramipexole differ markedly in their plasma protein binding however have related half-lives and have to be taken orally a quantity of occasions per day. Rotigotine is quickly and extensively metabolized by a number of P450s in the liver, and glucuronidated and sulfated metabolites are excreted within the urine (71%) and feces (23%). Aripiprazole has been shown to be beneficial in a couple of small trials with a discount in chorea equal to that noted with tetrabenazine. Controlled-release formulations are available to decrease the variety of daily doses required and prolong therapeutic plasma concentrations. This preparation dissolves instantly and releases the lively medication inside 30 minutes, with different pharmacokinetic parameters just like the oral preparations. Drugs for Huntington Disease Tetrabenazine is reasonably absorbed (75%) following oral administration, with no effect of meals. Tetrabenazine has a half-life of 10 hours, with the half-life of the lively metabolite 4�8 hours, requiring that the drug be taken 2�3 times per day. The pharmacokinetic profile of deutetrabenazine is similar to that of tetrabenazine. Central nervous system results embrace depression, anxiety, agitation, insomnia, hallucinations, and confusion, notably in the aged, and may be attributed to enhanced mesolimbic and mesocortical dopaminergic activity. The tricyclic antidepressants or serotonin selective reuptake inhibitors (Chapter 17) could also be used for melancholy, however the latter might worsen motor signs. As the disease progresses, even with continued remedy, the period of therapeutic activity from each dose decreases. This is named the "wearing-off " impact, and heaps of sufferers fluctuate in their response between mobility and immobility, generally known as the "on-off " effect. In addition, after 5 years of continued drug remedy, as many as 75% of sufferers experience dose-related dyskinesias, characterised by chorea and dystonia, inadequate therapeutic responses, and toxicity at subtherapeutic doses. Tolcapone has been taken off the market in Canada, however not the United States, as a consequence of induced deadly hepatotoxicity. Baseline liver function checks should be carried out earlier than starting tolcapone and should be repeated throughout remedy. Combinations of those compounds may induce "serotonin syndrome," a serious situation characterized by confusion, agitation, rigidity, shivering, autonomic instability, myoclonus, coma, nausea, diarrhea, diaphoresis, flushing, and even death. The compulsive behaviors might replicate stimulation of the midbrain dopaminergic ventral tegmental-nucleus accumbens pathway thought to mediate addictive behaviors (Chapter 13). The muscarinic receptor antagonists all trigger typical anticholinergic effects, as mentioned in Chapter eight. Amantadine may produce hallucinations and confusion, nausea, dizziness, dry mouth, and an erythematous rash of the lower extremities. Symptoms might worsen dramatically whether it is discontinued, and amantadine must be used with caution in sufferers with congestive heart disease or acute angle-closure glaucoma.
400 mg sevelamer free shipping
A, Computed tomographic scan reveals a big tumor apparent in the best liver and lengthening properly into the left (top arrow). D, Celiac axis angiogram shows the arterial supply to the tumor arising from the left hepatic artery. E, An accent proper hepatic artery is revealed to arise from the superior mesenteric trunk (arrow). F, Late-phase portogram obtained from selective splenic artery catheterization reveals tumor involvement of the best branch of the portal vein extending to the portal venous bifurcation (arrows). The tumor proved to be a main hepatocellular carcinoma, and remedy was by prolonged right hepatectomy. Note: Angiographic techniques at the moment are not often utilized in prognosis, however the pictures are retained for illustrative functions. The morphologic configuration of tumors on imaging studies has been proven to have a transparent relationship to subsequent resectability. Tumors that expand and compress surrounding tissues (pushing tumors) and tumors that are pedunculated and connected to the liver by a base of slender width (hanging tumors) are nearly always resectable, and they should be distinguished from tumors which are irregular on the margins and clearly invasive (Baer et al, 1989). In the early years of hepatic resection, the editor emeritus (Leslie H Blumgart) adopted and promoted a deliberate coverage of full investigation at laparotomy to assess resectability in all sufferers with solitary large liver tumors, supplied no positive proof of extrahepatic spread was obvious, patients have been in any other case fit for main surgical procedure, and the residual liver could be adequate. Of 22 sufferers with major liver cancer evaluated in an early examine, 13 patients have been explored, and all underwent E. Extended proper hepatectomy was done, and tumor clearance was obtained; hepatic vascular isolation was not used. Two of these thirteen sufferers had tumor embolization before surgery to cut back vascularity and tumor dimension. No intraoperative or in-hospital (30 day) deaths have been reported (Soreide et al, 1985). This early expertise has been replicated in subsequent studies (Vauthey et al, 1993) and in research by many other investigators. When oncologically indicated, nevertheless, an aggressive surgical coverage does seem justified, even in sufferers with massive solitary tumors. Ultrasound defines the connection between a colorectal metastasis and the veins on the hepatic vein confluence. A, Transverse ultrasound exhibits the metastasis (asterisk) making contact with the inferior vena cava (i) and proper hepatic vein (r). B, Oblique intercostal projection confirms that the right hepatic vein is compressed (arrow) but not invaded by tumor (asterisk). Transverse ultrasound reveals hilar cholangiocarcinoma on the confluence of the hepatic ducts. The portal vein confluence immediately under the tumor is unaffected, and the portal vein is free. The tumor extended into the proper hepatic duct, subsequently an extended proper hepatectomy was necessary. Other markers, significantly plasma neurotensin ranges (Collier et al, 1984) and vitamin B12 binding capability (Paradinas et al, 1982), are elevated with this tumor. More just lately, transplantation has emerged as an effective and viable remedy choice in sufferers with cirrhosis and restricted neoplastic illness, with the Milan standards now firmly established for guiding patient choice (Mazzaferro et al, 1996). A, Selective hepatic arteriogram exhibits a big main hepatocellular carcinoma (arrows). C, Selective splenic artery catheterization and late-phase splenoportogram present severe compromise of the proper branch of the portal vein (black arrow). Preoperative Preparation Preoperative preparation entails applicable antibiotic prophylaxis and correction of anemia and coagulopathy. Patients with a big history of lively cardiopulmonary disease should endure any indicated investigations and optimization earlier than undergoing resection. Adequate hemodynamic monitoring and amenities for fast transfusion ought to be obtainable, and the anesthesia staff ought to be ready for the potential of a thoracoabdominal incision, although this is not often needed. Bleeding throughout hepatic resection normally occurs throughout parenchymal transection and arises from the hepatic veins or vena cava. Thus, we routinely carry out a deliberate retrohepatic dissection of the minor and main hepatic veins before starting parenchymal transection, unless the tumor location and dimension prohibit this method and mandate an anterior strategy. To forestall air embolism, the dissection has historically been performed with the affected person in a 15 degree Trendelenburg place; however, this problem is exceedingly uncommon, and performing the resection with the affected person in neutral or reverse Trendelenberg place is also safe. A minimal intraoperative urine output (20-25 mL/hr) is tolerated till parenchymal transection is full (Cunningham et al, 1994; Melendez et al, 1998) (see Chapter 24).
Diseases
- Cleft lip palate abnormal thumbs microcephaly
- Growth delay, constitutional
- Dwarfism lethal type advanced bone age
- Adams Nance syndrome
- Rubella
- Glutaricaciduria II
- Renal carcinoma, familial
- Gen?e-Wiedemann syndrome
- Epilepsy benign neonatal familial 1
- Perilymphatic fistula
Cheap sevelamer 400 mg with visa
The main portal trunk is exposed and dissected superiorly, until the left branch is revealed and preserved. A renal pedicle clamp is passed gently around the proper portal vein beneath direct imaginative and prescient. Special care ought to be taken to not harm the primary posterior department of the proper portal vein, which comes off early and posteroinferiorly to provide the proper portion of the caudate lobe. If any issue is encountered in encircling the best portal vein, this branch must be individually ligated and divided earlier than any instrument is handed around the best portal trunk. It is sweet apply to place two retaining prolene sutures to secure the vein before dividing it to prevent retraction. These sutures should be left with the needle in place and are used to oversew the stump after the vein has been divided. Because it might be troublesome to get hold of a transparent view of the best hepatic duct and its tributaries for dissection and ligation extrahepatically, these buildings are best left intact and divided intrahepatically at parenchymal dissection. However, if extrahepatic control of the best hepatic duct is necessary, most often for oncologic functions, it could be dissected out at this point. This maneuver opens the umbilical fissure and allows better publicity of the subhepatic house. Absorbable suture materials ought to be used to forestall permanent suture appearing as a nidus for future stone formation or infection. If issue is encountered in passing a suture round the best hepatic duct, it may be divided beneath direct visualization and subsequently oversewn with a 4-0 absorbable suture. Often, the ducts draining the proper anterior and posterior sections are discovered getting into the confluence separately, or the proper posterior sectional duct might drain into the left hepatic duct (see Chapter 2). In such instances, both these main sectional ducts ought to be individually identified and secured. This approach is most helpful for right-sided tumors located peripherally away from the hilus, which allows its use with out compromising tumor clearance. This method allows the surgeon to dissect and clamp the required sheaths early within the operation to higher outline the phase or segments to be eliminated. Essentially, the method depends on intrahepatic definition and control of the portal triads of the segments being removed. By eliminating hilar dissection, pedicle ligation saves time and prevents potential damage to the contralateral vessels and bile ducts. Other than this cautionary notice, the technique is nearly equivalent to that described by Launois (see later). This technique also can be utilized to management the left sheath, however we choose to dissect the constructions throughout the umbilical fissure, as mentioned later. Pedicle Ligation An important various to extrahepatic dissection of the hilar structures is the pedicle ligation technique that makes use of the intrahepatic method first described in Japan by Takasaki and colleagues (1986a, 1986b) and then in the West by Launois (1994) Exposure and Control of Right Hepatic Vein the best hepatic vein may be managed from inside the liver throughout hepatic parenchymal transection, or it could be isolated and divided extrahepatically before proceeding with division of the liver tissue. The liver has been mobilized from the inferior vena cava by division of the retrohepatic veins mendacity behind the caudate course of. Hepatotomies have been made within the area of the gallbladder fossa and the caudate course of. The curved double-headed arrows point out the websites of the hepatotomies above and beneath the porta hepatis. B, A vessel loop is drawn about the best pedicle and pulled to the left to defend the left pedicular buildings throughout control and transection of the proper primary sheath. The vessel loop is drawn firmly to the left, and the pedicle is split utilizing the stapler, as shown in D. F, Operative photograph exhibits division of the best portal vein pedicle, which is encircled by a red vessel loop pulled to the left. B, Photograph illustrates insertion of the index finger via a hepatotomy in the caudate lobe, the place it merges with the bottom of the gallbladder fossa to isolate the proper portal pedicle. B, this illustration reveals the approach to the proper posterior pedicle (right lateral pedicle). To management the best hepatic vein extrahepatically, the liver is turned to the left by incising the right coronary ligament, proper triangular ligament, and inferior peritoneal attachements. If the surgeon chooses to accomplish that, an umbilical tape can be handed quite easily under the liver, between the inferior floor of the liver and the best renal vein. It is dangerous to persist through an abdominal incision in an try to mobilize a rigid right lobe of a liver containing a large tumor, as a end result of the right hepatic vein might tear posteriorly. Mobilization and control of the right hepatic vein are sometimes carried out before influx occlusion.
Buy 400 mg sevelamer amex
Bile duct injury could be decreased by performing intraoperative cholangiography, which nonetheless represents the gold standard for finding out the biliary tract anatomy in addition to for guiding reconstruction in circumstances of bile duct resection. Intrahepatic Biliary Tree Integrity It is essential to affirm biliary tree integrity after suspicion of damage throughout surgical dissection to keep away from postoperative morbidity and the ensuing want for invasive procedures and even redo surgical procedure. This data is essential for planning the resection, and in this sense, Proper Drainage of Bile Duct Stump the correct biliary drainage of the remnant liver once a bile duct has been resected is important. This is particularly true in sufferers operated on for perihilar cholangiocarinoma. Since this strategy reduces the rate of main hepatectomies, could be additionally debated the true need of interventions such as preoperative portal vein embolization, which are adopted to prevent liver failure after removal of great quantities of liver parenchyma (Torzilli et al, 2009c). However, this approach to liver resection, which permits the mix of widened indications and a excessive normal of safety, demands large incisions with extensive mobilization and sophisticated dissection planes. These necessities run counter to the pattern to use smaller incisions, corresponding to with the anterior method, with or with out the hanging maneuver (Liu et al, 2006; Ogata et al, 2007). Therefore surgery can nonetheless be considered the remedy of selection for many liver tumors, whatever the development and progress in different local treatments, similar to ablation therapies and intravascular procedures. Currently, nevertheless, these modalities stay pricey, provide little extra medical benefit, and are characterised by a posh "plug and play," which additional limits their usefulness. Agrawal N, et al: the routine use of intraoperative ultrasound in patients with colorectal cancer improves the detection of hepatic metastases, Colorectal Dis eight:192�194, 2006. Arita J, et al: Usefulness of contrast-enhanced intraoperative ultrasound using Sonazoid in sufferers with hepatocellular carcinoma, Ann Surg 254:992�999, 2011. Beller S, et al: Feasibility of navigated resection of liver tumors utilizing multiplanar visualization of intraoperative third-dimensional ultrasound knowledge, Ann Surg 246:288�294, 2007. Beller S, et al: Upgrade of an optical navigation system with a everlasting electromagnetic position management: a primary step in path of "navigated control" for liver surgery, J Hepatobiliary Pancreat Surg sixteen:165�170, 2009. Cerwenka H, et al: Is intraoperative ultrasonography throughout partial hepatectomy still needed within the age of magnetic resonance imaging Cucchetti A, et al: Recovery from liver failure after hepatectomy for hepato-cellular carcinoma in cirrhosis: which means for the Model of End-stage Liver Disease, J Am Coll Surg 203:670�676, 2006. Curro G, et al: Ultrasound-guided radiofrequency-assisted segmental liver resection: a brand new method, Ann Surg 250:229�233, 2009. Eguchi S, et al: Comparison of the outcomes between an anatomical subsegmentectomy and a non-anatomical minor hepatectomy for single hepato-cellular carcinomas based mostly on a Japanese nationwide survey, Surgery 143:469�475, 2008. Gotoh N, et al: A novel image-guided surgical procedure of hepatocellular carcinoma by indocyanine green fluorescence imaging navigation, J Surg Oncol 100:75�79, 2009. Hamada H, et al: Efficacy of a navigation system in neuro-endoscopic surgery, Minim Invasive Neurosurg 48:197�201, 2005. Hasegawa K, et al: Prognostic impact of anatomic resection for hepatocellular carcinoma, Ann Surg 242:252�259, 2005. Hata S, et al: Value of visual inspection, bimanual palpation, and intraoperative ultrasonography throughout hepatic resection for liver metastases of colorectal carcinoma, World J Surg 35:2779�2787, 2011. Hohlweg-Majert B, et al: Navigational maxillofacial surgery using digital models, World J Surg 29:1530�1538, 2005. Imamura H, et al: One thousand fifty-six consecutive hepatectomies without mortality in 8 years, Arch Surg 138:198�206, 2003. Inoue Y, et al: Anatomical liver resections guided by third-dimensional parenchymal staining utilizing fusion indocyanine green fluorescence imaging, Ann Surg 262(1):105�111, 2015. International Consensus Group for Hepatocellular Carcinoma: Pathologic diagnosis of early hepatocellular carcinoma: a report of the International Consensus Group for Hepatocellular Neoplasia, Hepatology forty nine:658�664, 2009. Ishizawa T, et al: Real-time identification of liver cancers through the use of indocyanine green fluorescent imaging, Cancer 115:2491�2504, 2009. Jaeck D, et al: A two-stage hepatectomy procedure mixed with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases, Ann Surg 240:1037�1049, 2004. Kaibori M, et al: Comparison of limited and anatomic hepatic resection for hepatocellular carcinoma with hepatitis C, Surgery 139:385�394, 2006. Kato K, et al: Intra-operative software of real-time tissue elastography for the prognosis of liver tumours, Liver Int 28:1264�1271, 2008. Kokudo N: Clinical application of fluorescence imaging of liver most cancers using indocyanine green, Liver Cancer 1(1):15�21, 2012. Kokudo N, et al: Management of latest hepatic nodules detected by intraoperative ultrasonography during hepatic resection for hepatocellular carcinoma, Surgery 119:634�640, 1996. Kudo M: New sonographic techniques for the diagnosis and remedy of hepatocellular carcinoma, Hepatol Res 37(Suppl 2):S193�S199, 2007.
Order sevelamer 400 mg with visa
Treg cells have the ability to suppress cytokine secretion, adhesion molecule expression, and costimulatory signaling. Animal fashions suggest that these cells play a crucial role in controlling immune activation (Baecher-Allan et al, 2001; Wood & Sakaguchi, 2003). The prevailing evidence means that Treg cells are aware of established inflammation, rather than serving a prophylactic position in preventing inflammation. However, harnessing the power of Treg cells to quell counteradaptive immune responses similar to rejection is an ongoing space of research in autoimmunity and alloimmunity (Juvet et al, 2014). Evolving Cellular Composition With Age A hallmark of immunity is its capacity to adapt primarily based on prior immune experience, such that initial immune responses are much less strong than anamnestic responses. While people age, prior immune experience grows, manifest in an noticed loss of naive T and B cells and a commensurate accumulation of cells expressing a reminiscence phenotype. This transition is accentuated by physiologic thymic atrophy, which slows the manufacturing of naive T cells (Gruver et al, 2007). By using established markers of resting naive T cells and reminiscence cell activation, four T-cell subpopulations have been described that appear to differ when it comes to their degree of antigen experience, prior activation historical past, and migratory capabilities (Sallusto et al, 1999). These could be basically outlined as naive T cells, effector memory T cells, central memory T cells, and terminally differentiated effector cells. This is increasingly necessary because lots of the molecules targeted in transplantation, significantly costimulatory molecules, are altered with immune expertise such that optimum immune administration is more probably to require cognizance of these modifications. Humoral Immunity B cells acknowledge antigen in its native, unprocessed form (Cambier et al, 1994). When antigen binds to two cell surface antibodies, the antibodies are introduced together in a course of often recognized as cross-linking, stimulating B-cell proliferation and differentiation into an antibody-secreting plasma cell. B cells also have the power to internalize antigen certain to floor immunoglobulins and process them for presentation to T cells together with costimulation molecules (Lederman et al, 1992). The fundamental antibody construction consists of two equivalent heavy chains and two identical gentle chains. The kind of heavy chain used dictates the immunoglobulin (Ig) sort: IgM, IgG, IgA, IgE, or IgD. The general structure of the antibody leads to two similar antigen-binding websites and a typical area, the Fc portion. Bound antibody triggers activation of the complement cascade (Baldwin et al, 1995). In addition, most phagocytic cells have receptors for the Fc portion of IgG, allowing them to actively engulf antibody-coated cells. Isotype switching is the process of shifting from the preliminary heavy-chain IgM to one of four sorts to enhance operate and specialization of the secreted antibody. IgG is the most significant soluble mediator of opsonization and is the dominant antibody produced in response to alloantigen. IgA is important in mucosal immunity, IgE is concerned in mast cell�mediated immunity, and IgD is primarily cell certain. The resultant B-cell clones have altered antigen affinity, thus the time period affinity maturation (Griffiths et al, 1984). Clones which have greater affinity for the target antigen have a selective survival advantage and form the idea for a extra vigorous response on reexposure to the antigen. The kind of costimulatory sign acquired by the lymphocyte determines whether the cell will become activated, stay quiescent, die, or turn out to be resistant to subsequent immune stimulation. The biology of T-cell costimulation is substantially more developed than that of B-cell costimulation. Therefore, sites of trauma that recruit platelets create an environment of activating costimulatory molecules, thereby bridging the innate and bought immune techniques (Czapiga et al, 2004). In addition to cytokines, other soluble mediators of inflammation are able to selling increased blood circulate and improved exposure of an area of harm to innate and purchased immune parts. Many of those cells are crossreactive with antigen encountered during prior viral exposures, and even with autoantigens, as in the case of autoimmune illness. This is named heterologous immunity and results in a situation whereby recipients have allospecific memory without having been exposed to the alloantigen (Adams et al, 2003a, 2003b). In addition, adhesion and costimulation molecules are upregulated perioperatively (Hoffmann et al, 2002; Takada et al, 1997). Initial T-cell binding to donor cells is nonspecific, mediated by adhesion molecules upregulated during donor cell activation (Fuggle & Koo, 1998).
Cheap sevelamer 800 mg on line
Whereas radiologic evaluation as quickly as required invasive investigations in many cases, it can now present complete, noninvasive assessment of the liver, together with the biliary tree, the arterial and venous anatomy, and the intrahepatic and extrahepatic disease extent in the case of malignant disease (see Chapters 15, 18, and 19). Indeed, for sure tumors, traditional imaging findings are actually thought-about pathognomonic and have supplanted the necessity for a biopsy. Specific examples on this regard embody liver hemangiomata and focal nodular hyperplasia (see Chapter 19) and the rules for the analysis of hepatocellular carcinoma (Bruix & Sherman, 2005). Going ahead, advances in imaging expertise likely to affect the practice of hepatic resectional surgical procedure embody computer-aided reconstruction, functional imaging, and intraoperative navigation (Cherqui & Belghiti, 2009; Chopra et al, 2010). Advances in imaging have additionally performed a significant function in postoperative administration, particularly in diagnosing and treating postoperative complications. During the past several years, the marked reduction in operative mortality after hepatic resection has seemingly occurred with little apparent change in morbidity. This statement suggests an total improvement in the capacity to salvage sufferers who experience important issues. The ready availability of high-quality imaging and a heightened sense of consciousness of the perioperative issues that may occur have led to earlier detection of problems. These adjustments, combined with the power to manage many problems percutaneously or endoscopically, somewhat than operatively, have clearly had a major influence on perioperative consequence. The descriptions herein replicate the current cutting-edge, built upon the collective contributions of many pioneering surgeons over the previous several decades and continuing to the current. The methods and approaches discussed embody, to a point, the biases of the authors; nonetheless, the overriding theme is always adherence to greatest ideas of hepatic resection surgical procedure, and various viewpoints should be thought of the place appropriate. Bruix J, Sherman M, Practice Guidelines Committee, American Association for the Study of Liver Diseases: Management of hepatocellular carcinoma, Hepatology 42(5):1208�1236, 2005. Lortat-Jacob J, Robert H: [Well-defined method for proper hepatectomy], Presse Med 60(26):549�551, 1952. Makuuchi M, et al: Preoperative transcatheter embolization of the portal venous department for patients receiving extended lobectomy because of the bile duct carcinoma, J Jpn Surg Assoc 45:1558�1564, 1984. Valle J, et al: Cisplatin plus gemcitabine versus gemcitabine for biliary tract most cancers, N Engl J Med 362(14):127�381, 2010. Maithel Hepatic resection could also be needed for the remedy of all kinds of situations involving the liver and biliary tract (Box 103B. The most common indication for partial hepatectomy is elimination of metastatic lesions (see Chapters 92-94), which may additionally embrace elimination of benign and malignant main tumors of the liver and biliary tract (Chapters forty seven, 49-51, 90A, 91, and 95). In addition, hepatic resection could additionally be used to treat complicated or symptomatic cystic illness of the liver (see Chapter 90B), to allow entry for the restore of select benign biliary strictures (Chapter 42), and sometimes to handle hepatic trauma (see Chapter 122). More just lately, liver resection in dwelling donors has been utilized in liver transplantation (see Chapter 104). A mastery of intrahepatic anatomy, supplemented by means of intraoperative ultrasound (Bismuth & Castaing, 1984; Castaing et al, 1985; Scheele, 1989) (see Chapters 23 and 110) to establish intrahepatic structures is paramount to secure resections. Commonly performed segmental resections, together with caudate lobe resection, are briefly described as properly. A more detailed description of segment-oriented resection of the liver is provided in Chapter 108B. Special considerations in liver resection mentioned in this chapter embody patients with cirrhosis (see Chapter 103D) and first extrahepatic biliary most cancers (Chapter 103C). In patients with cirrhosis, the presence of portal hypertension and a concomitant useful deficit of the long run liver remnant might complicate intraoperative and postoperative administration (see Chapter 108A). Liver resection for gallbladder carcinoma and hilar cholangiocarcinoma may be especially troublesome within the presence of biliary obstruction, bacterial contamination, and infection. In certain circumstances of complex benign biliary strictures, especially when related to ipsilateral liver atrophy, liver resection may be required (see Chapter 42). Other benign biliary circumstances which will necessitate resection include intrahepatic stones associated with recurrent pyogenic cholangitis (see Chapter 39) and Caroli disease, a congenital cystic disease of the liver (see Chapter 46). Malignant Disease When partial hepatectomy for malignant tumors is carried out, the tenet is to get hold of unfavorable margins of resection while sustaining affected person security. Ideally, the closest margin distance from the tumor edge should be roughly 1 cm (Are et al, 2007). Furthermore, an effort ought to all the time be made to carry out parenchyma-sparing resections without sacrificing oncologic efficacy. Consequently, wedge resections can carry an unacceptable native recurrence price (DeMatteo et al, 2000; Gall & Scheele, 1986), though this has not been universally noticed (Zorzi et al, 2006). Another factor that may compromise wedge resections is that the liver tends to fracture at the interface between tumor and regular parenchyma.