
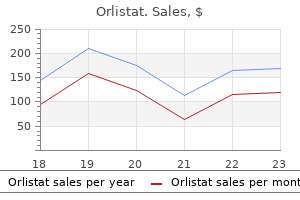
Orlistat dosages: 120 mg, 60 mg
Orlistat packs: 10 caps, 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Buy orlistat without prescription
The principal features of sensory-ataxic gait are the brusqueness of movement of the legs and stamping of the toes because the foot is forcibly brought down onto the ground (apparently to detect the location of the foot as an alternative to proprioception). The feet are positioned far apart to right the instability, and patients fastidiously watch both the bottom and their legs. As they step out, their legs are flung abruptly forward and outward, in irregular steps of variable size and top. The body is held in a barely flexed position, and a few of the weight is supported on the cane that the severely ataxic patient usually carries. Such sufferers, when requested to stand with feet collectively and eyes closed, present tremendously increased swaying and usually, the totally expressed Romberg sign with falling off to one facet. Examination often discloses a loss of position sense within the toes and legs and usually of vibra tory sense as properly. The peripheral or central location of the sensory lesions could be additional determined by the state of the tendon reflexes. Walking with out the assist of a cane or the arm of a companion brings out a certain stiffness of the legs and firmness of the muscular tissues. The latter abnormality could also be analogous to positive supporting reactions observed in cats and canine following ablation of the anterior vermis; such animals react to pressure on the foot pad with an extensor thrust of the leg. The drunken patient totters, reels, ideas forward after which backward, appear ing each moment to be on the verge of shedding his bal ance and falling. As indicated above, the adjectives drunken and reeling are used frequently to describe the gait of cerebellar illness, but the similarities between them are only superficial. The severely intoxi cated patient reels or sways in many different instructions and seemingly makes little or no effort to right the staggering by watching his legs or the bottom, as occurs in cerebellar or sensory ataxia. Despite wide excursions of the body and deviation from the line of march, the drunken affected person might, for short distances, have the ability to stroll on a slender base and maintain his balance. In distinction, the patient with cerebellar gait has great issue in cor recting his steadiness if he sways or lurches too far to one aspect. Milder levels of the drunken gait extra closely resemble the gait dysfunction that follows loss of labyrin thine perform (see earlier discussion). Walking is accom plished by extreme flexion on the hip, the leg being lifted abnormally high to guarantee that the foot to clear the bottom. Foot drop may be unilateral or bilateral and occurs in diseases that have an result on the peripheral nerves of the legs or motor neurons in the spinal cord, similar to continual acquired neuropathies (diabetic, inflammatory, toxic, and nutritional), Charcot-Marie-Tooth illness (peroneal mus cular atrophy), progressive spinal muscular atrophy, and poliomyelitis. It may also be observed in sure kinds of muscular dystrophy during which the distal musculature of the limbs is involved. A explicit dysfunction of gait, also of peripheral origin and resembling steppage gait, could additionally be observed in sufferers with painful dysesthesias of the soles of the feet. Because of the exquisite ache evoked by tactile stimulation of the feet, the patient treads gingerly, as if walking naked foot on hot sand or pavement, with the toes rotated in such a means as to limit contact with their most painful parts. The ordinary cause is one of the painful peripheral neuropa thies (most often alcoholic-nutritional but also poisonous and amyloid types), causalgia, or erythromelalgia. This dysfunction of gait can be seen in quite a lot of continual spinal wire diseases involving the dorsolateral and ventral tracts, most often multiple sclerosis, but in addition including syringomyelia, any kind of continual meningomyelitis, subacute mixed system disease of each the pernicious anemia and nonpernicious anemia sorts, spinal cord compression or traumatic damage, adrenomyeloneuropathy, and familial types of effects of posterior col umn disease are added, giving rise to a mixed gait disturbance-a spinal spastic ataxia, attribute of a number of sclerosis and certain spinal cord degenerations corresponding to Friedreich ataxia. Frequently in these diseases, the Parki nsonian and Festinati ng Gait Diminished or absent arm swing, ahead bent torso, quick or shuffling steps, turning en bloc, hesitation in beginning to walk, shuffling, or "freezing" when encounter ing doorways or different obstacles are the options of the parkinsonian gait. The steps are short, and the toes barely clear the ground as the affected person shuffles alongside. Once walking has began, the higher part of the body advances forward of the lower half, and the patient is impelled to take more and more short and speedy steps as if trying to catch up to his middle of gravity. The steps turn into more and more fast, and the affected person might easily break into a trot and collide with an impediment or fall if not assisted. The leg tends to rotate outward to describe a semicircle, first away from after which towards the trunk (circumduction). The foot scrapes the floor, contact being made by the toe and outer sole of the foot. One can recognize a spastic gait by the sound of gradual, rhythmic scuffing of the foot and sporting of the medial toe of the shoe. This kind of gait disorder is most frequently a sequela of stroke or trauma but may result from any situation that damages the cor ticospinal pathway on one facet.
Order genuine orlistat on line
In probably the most severe instances and those refractory to treatment with botulinum toxin, a mixed sectioning of the spinal accessory nerve and of the first three cervi cal motor roots bilaterally has been successful in lowering spasm of the muscular tissues without totally paralyzing them. Considerable relief has been achieved for so lengthy as 6 years in one-third to one-half of instances treated in this means (Krauss et al; Ford et al). Blepharospasm Patients in mid and late grownup life, predominantly women, might current with the complaint of inabil ity to keep their eyes open that might be a manifestation of involuntary closure of the eyelids. Any attempt to have a glance at a person or object is related to a persistent tonic, symmetric spasm of the eyelids. During conversation, the patient struggles to overcome the spasms and is distracted by them. Reading and watching tv are unimaginable at some occasions however surprisingly easy at others. Jankovic and Orman in a survey of 250 such sufferers found that seventy five % pro gressed in severity through the years to the purpose, in about 1 5 % of circumstances, of constructing the sufferers functionally blind. Some cases of blepharospasm are a compo nent of the Meige syndrome that includes jaw spasms (see next section). However, the spasms persist in dim mild and even after anesthesia of the cor neas. No neuropathologic lesion or neurochemical profile has been established in any of those problems (Marsden et al; see additionally Hallett). Finally, eye closure with fluttering of the lids in patients with a excessive degree of suggestibility is normally indicative of a psychological disorder. Blepharospasm induced by pain from ocular situations corresponding to iritis and rosacea of the eyelids has already been talked about. Lingual, Facial, and Oromandibular Spasms these special kinds of involuntary movements also appear in later grownup life, with a peak age of onset within the sixth decade. The most typical kind is characterised by forceful opening of the jaw, retraction of the lips, spasm of the platysma, and protrusion of the tongue; or the j aw could also be clamped shut and the lips might purse. Common phrases for this situation are Meige syn drome, after the French neurologist who gave an early description of it, and Brueghel syndrome, due to the similarity of the grotesque grimace to that of a topic in a Brueghel portray known as De Gaper. Difficulty in speak ing and swallowing (spastic or spasmodic dysphonia) and blepharospasm are also frequently conjoined, and occasionally sufferers with these disorders develop torti collis or dystonia of the trunk and limbs. All these prolonged, forceful spasms of facial, tongue, and neck muscle tissue have followed the administration of pheno thiazine and butyrophenone medicine. More usually, nevertheless, the dyskinetic disorder induced by neuroleptics is a few what different, consisting of choreoathetotic chewing, lip smacking, and licking movements (tardive orofacial dyskinesia, rabbit-mouth syndrome; see later). Sometimes the blepharospasm disappears spontaneously (in thirteen p.c of the instances in the series of Jankovic and Orman). Thermolytic destruc tion of a part of the fibers within the branches of the facial nerves that innervate the orbicularis oculi muscular tissues is reserved for the most resistant and disabling circumstances. Reflex blepharospasm, as Fisher has referred to as this phenomenon, takes liberty with the term because it more in the character of an apraxia of opening of the lids. A homolateral blepharospasm has additionally been noticed with a small thalamomesencephalic infarct. In one patient there have been foci of neuro nal loss in the striatum (Altrocchi and Forno); one other affected person confirmed a lack of nerve cells and the presence of Lewy bodies in the substantia nigra and related nuclei (Kulisevsky et al); each are of unsure significance. A type of focal dystonia that impacts solely the jaw mus cles has been described (masticatory spasm of Romberg); a similar dystonia may be a part of orofacial and generalized dystonias. In the circumstances described by Thompson and colleagues, the issue started with brief periods of spasm of the pterygoid or masseter muscle on one facet. Early on, the differential analysis includes bruxism, hemifacial spasm, the odd rhythmic jaw transfer ments associated with Whipple disease, and tetanus. As the illness progresses, forced opening of the mouth and lateral deviation of the jaw may final for days and adven titious lingual actions could additionally be added. In patients with Parkinson illness, progressive supranuclear palsy, or Wilson disease and with other lesions in the rostral brainstem, light closure of the eyelids could induce blepha rospasm and an incapability to open the eyelids voluntarily. We have seen an occasion of blepharospasm as a part of paraneoplastic midbrain encephalitis, and there have been a quantity of reviews of it with autoimmune disease similar to systemic lupus however the mechanism in these cases is as obscure as for the idiopathic variety. High doses of benztropine and associated anticholinergic medicine may be useful, however are not pretty a lot as good as botulinum toxin therapy.
120 mg orlistat with amex
The etiologies of status epilepticus range amongst age teams however all the fundamental causes of seizures are capable of produce the syndrome. Nonetheless, a long-acting antiepileptic similar to phe nytoin have to be given irrunediately after a diazepine has managed the initial seizures. An alternative is the water soluble drug fosphenytoin, which is run in the identical dose equivalents as phenytoin but could be injected at twice the maximum fee. Moreover, it could be given intramuscularly in instances where venous entry is difficult. However, the delay in hepatic conversion of fosphenyt oin to active phenytoin makes the latency of scientific impact roughly the identical for each medicine. If this fails to suppress the seizures and standing has continued for 20 to 30 min, an endotracheal tube must be inserted and 02 administered. Several approaches have been suggested to management standing epilepticus that persists after these efforts. A normal saline infusion is begun and a bolus of glucose thiamine is given (with (0. This routine of midazolam and phenytoin may be major tained for several days with out maj or unwell effect in pre 20 mg has been given; 0. More rapid administration risks hypotension Immediately thereafter, a loading dose and heart block; consequently, it is strongly recommended that the blood strain and electrocardiogram be monitored in the course of the infusion. In the field, emergency medical technicians can administer lorazepam drug or midazolam. Attesting to the benefit of rapidly treating seizures, Silbergleit and colleagues have shown that intramuscular administra tion is slightly superior to the intravenous route merely of its clinically longer period of motion (see Table 16-8). Prolonged use of propofol might pre cipitate hypertriglyceridemia-associated pancreatitis or a fatal shock and acidosis ("propofol syndrome"). Valproate and levetiracetam can be found as intrave nous preparations, making them appropriate for administra viously healthy p atients. Another reliable strategy 5 mg/kg, one hundred mg/min till the sei zures cease or a complete dose of 20 mg / kg is reached; a protracted is infusion of either pentobarbital, starting with or phenobarbital, at a rate of interval of stupor should be anticipated after. Hypotension often limits the continued use of the barbiturates, but Parviainen and colleagues have been capable of manage this prob lem by fluid infusions, dopamine, and neosynephrine. The most popular medicines for this function have been pen tobarbital or propofol, which, regardless of their reasonable efficacy as major anticonvulsants, are easier to man age than the alternative inhalational anesthetic agents. Midazolam could also be most well-liked among the diazepines for transmucosal use as a outcome of it produces somewhat much less respiratory depression than the others in the class and has been simpler at controlling seizures based on a study by Mcintyre and colleagues. These approaches have discovered their primary use in children with frequent seizures who reside in super vised environments, where a nurse or father or mother is available to administer the medicine. Absence status should be managed by intravenous lorazepam, valproic acid, or each, followed by ethosuxi mide. Nonconvulsive generalized status is handled along the lines of grand mal standing, normally stopping short of utilizing anesthetic brokers (see Meierkord). In the case of epilepsia partialis continua, typically a troublesome situation phenomenon and the danger of overuse of medicines that may produce stupor. The patient must be involved by means of figuring out how troubling the movements are to him. Every 12 to 2 mg/kg/h, 24 h, the rate of infusion is slowed to decide whether or not the seizures have stopped. However, a couple of sufferers in this predica ment have survived and woke up, even at instances with minimal neurologic harm depending on the underly ing trigger. Halothane has been comparatively ineffective as an anticonvulsant, but ether, although impractical, has in the past been effective in some. At these facilities, it has been estimated that approximately 25 % of all sufferers with epilepsy are c andidates for surgical therapy and more than half of those may profit from extirpation of the epileptic cortical focus. With increas ing experience and standardized approaches, especially in patients with temporal lobe epilepsy, it has been sug gested that many patients are ready too lengthy before the surgical possibility. Ketarnine infusions have been a last resort, together with a midazolam infusion. With failure of aggressive anticonvulsant and anesthetic therapy, there could also be a temptation to paralyze all muscular activity, an effect easily attained with drugs similar to pancuronium, while neglecting the underlying seizures. The use of neuromuscular blocking medication and not using a concomitant try and suppress seizure activity is inadvisable. In the associated however less-serious condition of 60 p.c of patients with focal seizures will respond to a conventional anticonvulsant, but that among the the rest, few will reply to the addition of a second or third drug.
Cheap generic orlistat uk
A study of aged twins by McClearn and colleagues has shed further gentle on the difficulty; even in twins who were older than eighty years of age, a substantial part (an estimated with the exception of the pathologically developmentally delayed (Chaps. As to psychologic theories of intelligence, several have historically been held at different historical peri ods. One is the two-factor principle of Spearman, who noted that all the separate tests of cognitive talents correlated with one another, suggesting that a common factor 62 percent) of cognitive (gjactor) efficiency could be accounted for by genetic traits. These findings suggest that life expertise alters intelli gence, however in only a restricted means. There could be little doubt, therefore, that genetic endowment is the extra necessary factor-a view that was championed by Piercy and more lately by Herrnstein and Murray. The latter should be looked upon not because the sum of genetic and environmental fac tors but as the product of the two. As to the genetic mechanisms involved in the inheri tance of intelligence, a limited quantity is known. There is an excess of males with psychological retardation, and there are several well-characterized syndromes by which the inheritance of psychological retardation is X-linked as described in Chaps. Because not certainly one of the correla tions between subtests approached unity, he postulated that every take a look at measures not solely this common capability (com monly identified with intelligence) but additionally a subsidiary elements specific to the individual checks, which he desig nated the s components. A second principle, the multifactorial principle of Thurstone, proposed that intelligence consists of a selection of main mental talents, similar to memory, verbal facility, numerical capability, visuospatial perception, and capacity for downside fixing, all of them more or less equivalent. For Eysenck, intelligence exists in three types: biologic (the genetic component), social (development of the genetic component in relation to personal relationships), and a selection of particular talents subject to measurement by psychometric checks. Also notable is the considerably dif ferent patterns of subtest efficiency between women and men (males perform higher on subtests of spatial capacity and sure mathematical tasks). Males may be more likely to be affected by advantageous or aberrant genes on a single X chromosome, whereas females ben efit from the mosaic supplied by two X chromosomes. In some households, excessive intelligence segregates to certain people by way of an X-linked pattern. Further research will determine the validity of this view and its contribu intelligences, outlined as the flexibility to clear up problems or resolve difficulties and to be artistic throughout the par ticular subject. Several traces of evidence are marshaled in support of this parceling of separable expertise and talents: be a polygenic inheritance of mental traits. Each of these entities appears to have a genetic foundation in as far as musical, artistic, mathematical, and athletic capacity often runs in families, but their full growth is influenced by environmental elements. There are only limited data relating to the very best ranges of intelligence recognized as genius. One of the main theories has been that of Piaget, who proposed that that is completed in discrete phases related to age: sensorimotor, from 0 to 2 years; preconceptual thought, from 2 to 4 years; intuitive thought, from 4 to 7 years; concrete operations (concep tualization), from 7 to 11 years; and, lastly, the period of "formal operations" (logical or abstract thought), from 11 years on. This scheme implies that the capacity for logical thought, creating because it does based on an orderly timetable, is coded in the genes. One would suppose that in neurology, the place one is uncovered to so many diseases affecting the cerebrum, it might be attainable to verify certainly one of these a quantity of theories of intelligence and to determine the anatomy of this cogni tive entity. Presumably, the g factor of intelligence could be maximally impaired, by diffuse lesions, in propor tion to the mass of brain concerned, an concept expressed by Lashley as the "mass-action precept. Others disagree, claiming that no uni versal psychologic deficit can be linked to lesions have an result on ing specific components of the mind. According to Tomlinson and colleagues, who studied the results of vascular lesions within the growing older mind, lesions that involve greater than 50 mL of tissue trigger some basic reduction in performance, especially in pace and capability to remedy problems. Piercy, however, found correlations solely between specific intellectual deficits and lesions of particular components of the left and right hemispheres. The authors conclude from experience and from proof supplied by neurologic studies that intelligence is a mixture of multiple major abilities, each of which seems to be inherited and each of which has a sep arate however as yet poorly delineated anatomy. These are integral to ideation and problem solving and are largely absent in the developmentally delayed and misplaced early in dementing illnesses. It is expressed in thinking and abstract rea soning and is operative provided that the connections between the frontal lobes and other components of the mind are intact. Attention, drive, and motivation are noncognitive psy chologic attributes of fundamental significance, the pre cise anatomy and physiology of which remain to be identified however are largely generated in the frontal and prefrontal area. It can be attainable, if not likely, that the associative areas of the cerebrum are engaged in the apperception of sensory experiences and their manipula tion in symbolic type. This applies equally to the power to relate thoughts to each other and to saved ideas, however right here, reminiscence plays a central role.
Buy orlistat 120mg cheap
As many as three or 4 assaults could happen each week, leav ing the scalp on one aspect constantly tender. An even more difficult medical problem is posed by migraine that lapses into a condition of daily or just about extreme con tinuous headache (status migrainosus). The ache is initially unilateral, later more generalized, more or less throbbing, but with a constant superimposed ache and is disabling; vomiting or nausea is frequent on the outset however abates. Most of these circumstances in our expertise have turned out to be simply instances of aseptic meningitis that have precipitated migraine in vulnerable individu als. A more in depth syndrome was originally described by Bartleson, Swanson, and Whisnant under the title "A migrainous syndrome with cerebrospinal fluid pleocytosis". One-quarter of this group had a history of past migraine and an analogous number had a viral-like illne ss inside three weeks of the neu rologic drawback. The transient neurologic deficits have been mainly sensorimotor and aphasic; only 6 patients had visual symptoms. The patients have been asymptomatic between assaults and in none did the entire illness persist past 7 weeks. The causation and pathophysiology of this syndrome and its relation to migraine are obscure. The distinction between this syndrome and the recurrent aseptic meningitis of Mollaret and different chronic meningitic syndromes in addition to cere bral vasospasm or vasculitis is tough (see "Chronic Persistent and Recurrent Meningitis" in Chap. Tension and other emotional states, that are claimed by some migraineurs to precede their attacks, are so incon sistent as to be no extra than potential aggravating fac tors. The puzzle is how this genetic predisposition is translated periodically right into a regional neurologic deficit, unilateral headache, or each. For a few years, our excited about the pathogenesis of migraine was dominated by the views of Harold Wolff and others-that the headache was attributable to the distention and extreme pulsation of branches of the exterior carotid artery. Certainly, the throbbing, pulsating high quality of the headache and its relief by compression of the common carotid artery supported this view, as did the early observation of Graham and Wolff that the headache and amplitude of pulsation of the extracranial arteries diminished after the intravenous administration of ergotamine. The importance of vascular factors continues to be emphasised by more recent findings however not in the finest way envisaged by Wolff. For example, in a group of eleven patients with classic migraine, Olsen and colleagues, utilizing the xenon inhalation method, noted a regional reduction in cerebral circulation spreading forward from the occipital area in the course of the period when neurologic symptoms appear. They concluded that the reduction in blood circulate was consistent with the cortical spreading melancholy syndrome described below. In reference to the extracranial vessels, Iversen and associates, via ultrasonography, documented a dilatation of the superior temporal artery on the facet of the migraine in the course of the headache period. The identical dilatation in the center cerebral arteries has been inferred from observations with transcranial Doppler insonation. The complication of cerebral infarction is also in line with a vascular hypothesis, nevertheless it entails solely a tiny proportion of migraineurs. The unique opinion expressed by Wolff that a vascular factor is liable for the cranial pain of migraine can additionally be unconfirmed. The relationship between the vascular adjustments and evolving neurologic signs of migraine are notewor thy. Lashley, who plotted his own visual aura, calculated that the cortical impairment progressed at a price of 2 to three mm/min over the surface of the mind. Both of these events are intrigu ingly similar to the above-mentioned phenomenon of "spreading cortical despair," first observed by Leao in experimental animals. He demonstrated that a noxious stimulus applied to the rat cortex was followed by vaso constriction and slowly spreading waves of inhibition of the electrical exercise of cortical neurons, moving at a fee of approximately three mm/min. Lauritzen and Olesen attri bute both the aura and spreading oligemia to the unfold ing cortical depression, and appreciable work since then has corroborated this concept. An alternative, but not necessarily exclusive hypoth esis hyperlinks the aura and the painful phase of migraine via a neural mechanism originating within the trigemi nal nerve as proposed by Moskowitz. This relies on the innervation of extracranial and intracranial vessels by small unmyelinated fibers of the trigeminal nerve that subserve both ache and autonomic features (the "trigeminovascular" complex). The small molecules released from nerve end ings adjacent to the cortex would then incite spreading melancholy in this mannequin.
Buy cheap orlistat 60mg
Monitoring is finished by serial ultrasound from the tenth day onwards, till the signs of ovulation are noticed. It is characterised by ovarian enlargement, pleural and peritoneal effusion, oliguria, liver injury and thromboembolism. This causes decreased blood quantity and decreased albumin in addition to electrolyte levels. The increased vascular permeability is as a result of of prostaglandin, cytokines and development factors secreted by multiple growing follicles. It is an iatrogenic situation of increased vascular permeability resulting in exudation of fluids from the intravascular to the extracellular compartment. It has no anti-oestrogenic motion on the endometrium and the cervix-yields better pregnancy price. Urea, electrolyte estimation, serum protein degree Repeat ultrasound to monitor measurement of ovarian cyst and ascites. It is principally used within the palliative treatment of advanced breast cancer in postmenopausal ladies. Tamoxifen is efficient in main and secondary prevention of breast cancer; it prevents unfold to the other breast and recurrence by 50% and mortality by 25%. Side effects (two-fold increase) are scorching flushes, vaginal dryness (anti-E2 action), endometrial hyperplasia, polyp, endometrial carcinoma and sarcoma. Hyperglyceridaemia, deep venous thrombosis, ischaemic coronary heart disease and retinopathy are different issues to look forward to during tamoxifen therapy. Surgery is required if the ovarian cyst ruptures, undergoes torsion or haemorrhages. Aspiration of ovarian cyst, ascites, pleural and pericardial effusion could also be required. Aromatase Inhibitors Letrozole Letrozole (nonsteroidal aromatase inhibitor) is used in the induction of ovulation. Chapter 43 � Hormonal Therapy in Gynaecology 555 Dosage the dose is 10�20 mg twice day by day for no more than 5 years in breast most cancers because it turns into ineffective after that. Therapeutic Applications n Precautions Tamoxifen enhances the effects of warfarin. It is mandatory to monitor endometrial development by serial sonography and uterine aspiration. It is cardioprotective, maintains bone density and has no antagonistic impact on the endometrium not like tamoxifen. It is necessary to discontinue therapy before, throughout and after surgical procedure, to keep away from the danger of superficial and deep venous thrombosis. It is free from opposed effects on the breast, endometrium, ovary, liver and coagulation components. Usually the abortion takes place within 5 days of drug administration; nevertheless, one has to await 28 days to decide success. In 15% cases, when abortion fails to occur or is incomplete, or the patient continues to bleed, surgical evacuation turns into necessary. The drug is run within the form of three tablets (200 mg each), adopted by two tablets of misoprostol 200 �g, every orally or ideally vaginally forty eight h later. Lately, medical termination of being pregnant extended as much as 9 weeks of gestation with mifepristone and misoprostol has proved profitable. It is useful in ripening of the cervix previous to prostaglandin induction of mid-trimester abortion. Ectopic pregnancy-Mifepristone injected into the unruptured ectopic being pregnant causes its resolution (see Chapter 21 on Ectopic Gestation). Ten milligrams given inside 72 h of unprotected coitus is used as a post-coital contraception. It has some beneficial influence on shrinkage of fibroids and endometriosis (10�25 mg every day for 3 months). The drug binds to the receptors in the cell nucleus and blocks progesterone action on the goal organs. Administration of the drug (150 mg) through the first 3 days of the follicular phase has no effect on the menstrual cycle. It is a potent anti-androgen, and competes with dihydrotestosterone for intracellular androgen receptor sites-it inhibits its binding. Finasteride (Finast, fincar, fistide, finpecia) Finasteride is a aggressive inhibitor of the enzyme 5alpha reductase, which converts testosterone to dihydrotestosterone.
Generic orlistat 60 mg overnight delivery
Often this is the outcome of prema ture fixation on some item within the historical past or examination, closing the thoughts to different diagnostic considerations (the anchoring effect). The first diagnostic formulation must be considered solely a testable speculation, topic to modification when new items of knowledge are secured (anchoring heuristic). Should the illness be in a stage of transition, time will permit the full image to emerge and the diagnosis to be clarified. When several of the principle features of a illness in its typical kind are missing, another analysis should at all times be entertained. In general, nevertheless, one is extra prone to encounter uncommon manifestations of common illnesses than the typical manifestations of uncommon illnesses (a para phrasing of the consultant heuristic). There is little question that some clinicians are more proficient than others at solving tough scientific issues. To obtain professional efficiency in all areas, cognitive, musical, and athletic, a protracted period of targeted attention to the topic and to personal experi ence is required. There are a growing number of diseases, many medical and others surgical, for which specific therapy is now avail in a position; through advances in neuroscience, their quantity is steadily rising. Among essentially the most sweeping modifications, now that many infectious diseases of the nervous system are being addressed, have been entirely novel medica tions for stroke, a quantity of sclerosis, Parkinson illness, migraine, neuropathy, brain tumor and epilepsy. These therapies and the dosages, timing, and manner of admin istration of specific medication are thought of in later chap ters in relation to the description of individual diseases. There are, in addition, many ailments during which neu rologic function can be restored to a varying diploma by acceptable rehabilitation measures or by the considered use of therapeutic brokers. Claims for the effectiveness of a selected remedy primarily based on statistical evaluation of huge scale scientific research must be handled circumspectly. This is in part true because small albeit statistically significant effects may be of little consequence when applied to an individual patient. Here, the patient requires a skilled doctor to make judgments based mostly on partial or inadequate data. Even deciding actively to wait earlier than committing to an intervention displays wisdom and adheres to the dictum, "first, do no hurt". Even when no efficient treatment is possible, neurologic diagnosis is more than an mental pastime. The first step in the scientific examine of any disease process is its identification in the dwelling affected person. In closing this introductory chapter, a remark regarding the extraordinary burden of illnesses of the ner vous system throughout the world is appropriate. Furthermore, more so than in other fields, the promise of remedy or ameliora tion by new strategies similar to molecular biology, genetic therapy, and brain-computer interfaces has excited huge curiosity, for which cause features of the current scientific insights are included in acceptable sections. The evaluation and interpretation of data elicited by a care ful history and examination might show to be enough for prognosis. Special laboratory examinations then do not more than corroborate the medical impression. The purpose of the neurologist is to arrive at a ultimate analysis by suave evaluation of the scientific information aided by the least variety of laboratory procedures. Reflecting the limitations of laboratory diagnosis, in a carefully examined sequence of two. To inject a radiopaque substance, as in myelography, or a radioactive agent, as in radionuclide cisternography. Asymmetric lesions, significantly these near the tentorium or foramen magnum carry a higher threat of herniation precipitated by lumbar puncture. Consequently, the doctor should at all times judge the relevance and sig nificance of laboratory knowledge only within the context of clinical findings. Hence the neurologist must be familiar with all laboratory procedures relevant to neurologic disease, their reliability, and their hazards. Procedures that are pertinent to a specific symp tom complicated or category of disease-e. If the pressure proves to be very high-over 400 mm ideally on the left side for right-handed physicians, with hips and knees flexed, and the pinnacle as close to the knees as consolation permits. The puncture is often easiest to carry out at the L3-L4 interspace, which cor responds in lots of people to the axial aircraft of the iliac crests, or at the interspace above or under.
120 mg orlistat overnight delivery
The primary nuclei of the basal ganglia are represented in blue, as labeled on the proper. Diagram of the basal ganglia within the coronal airplane, illustrating the primary interconnections (see text for details). Whereas earlier concepts emphasized the serial connectivity of the basal gangli onic structures as talked about earlier, current proof signifies a corporation into a number of parallel basal ganglionic-cortical circuits. These circuits run parallel to the premotor pathway but stay separate anatomically and physiologically. At least five such anatomic circuits have been described, each projecting to a special por tion of the frontal lobe: (1) the prototypical motor circuit, converging on the premotor cortex; (2) the oculomo tor circuit, projecting onto the frontal eye fields; two prefrontal circuits: (3) one ending in the dorsolateral prefrontal and (4) the other on the lateral orbitofrontal cortex; and (5) a limbic circuit that initiatives to the ante rior cingulate and medial orbitofrontal cortex. An further and important characteristic of basal gangli onic construction is the nonequivalence of all parts of the striatum. Particular cell sorts and zones of cells inside this construction seem to mediate different aspects of motor control and to make the most of specific neurochemical transmitters, as detailed beneath under "Pharmacologic Considerations" (see additionally Albin et al and DeLong). This specialization has taken on further importance with the remark that one or another cell sort is destroyed preferentially in degenerative illnesses similar to Huntington chorea. Schematic illustration of main efferent and afferent connections of the basal ganglia. The blue traces incticate neurons with excitatory effects, whereas the black strains indicate inhibitory influences. It has been proposed on the idea of physiologic, lesional, and pharmacologic research, that there are two main efferent projections from the putamen; but these models are still in evolution. In most ways, the subthalamic nucleus and lateral pallidum operate as a single useful unit, (at least when it comes to the consequences of lesions in those locations on par kinsonian signs and the neurotransmitters concerned. The medial pallidum and reticular part of the substantia nigra could be viewed in an analogous unitary way, sharing the identical input and output patterns. Within the indirect path method, an internal loop is created by projections from the subthalamic nucleus to the medial phase of the palli dum and pars reticulata. A second offshoot of the indirect pathway consists of projections from the lateral pallidum to the medial pallidonigral output nuclei. From the inner pallidum, two bundles of fibers attain the thalamus-the ansa lenticularis and the fas ciculus lenticularis. The ansa sweeps across the inside capsule; the fasciculus traverses the internal capsule in numerous small fascicles after which continues medially and caudally to be part of the ansa in the prerubral field. Both of those fiber bundles be part of the thalamic fasciculus, which then contains not solely the pallidothalamic projections however additionally mesothalamic, rubrothalamic, and dentatothalamic ones. These projections are directed to separate targets in the ventrolateral nucleus of the thalamus and to a lesser extent within the ventral anterior and intralaminar thalamic nuclei. The centromedian nucleus of the intralaminar group initiatives again to the putamen and, through the parafas cicular nucleus, to the caudate. A main projection from the ventral thalamic nuclei to the ipsilateral premotor cortex completes the massive cortical-striatal-pallidal-tha lamic-cortical motor loop, with conservation of the somatotopic arrangement of motor fibers, once more empha sizing the nexus of motor control on the thalamic nuclei. Physiologic Considerations In easiest physiologic phrases, Denny-Brown and Yanagisawa, who studied the consequences of ablation of indi vidual extrapyramidal constructions in monkeys, concluded that the basal ganglia perform as a sort of clearinghouse the place, throughout an supposed or projected movement, one set of actions is facilitated and all other pointless ones are suppressed. They used the analogy of the basal ganglia as a brake or swap, the tonic inhibitory ("brake") motion preventing target constructions from producing unwanted motor exercise and the "change" operate referring to the capacity of the basal ganglia to choose which of many avail ready motor packages might be active at any given time. Still different theoretical constructs give attention to the function of the basal ganglia within the initiation, sequencing, and modulation of motor activity ("motor programming"). Also, it seems that the basal ganglia participate in the constant priming of the motor system, enabling the speedy execution of motor acts with out premeditation-e. In most methods, these conceptualizations restate the same notions of steadiness and selectivity imparted to all motor actions by the basal ganglia. Physiologic evidence indicates that a balanced func tional structure, one excitatory and the opposite inhibi tory, is operative within the particular person circuits. The direct striatomedial pallidonigral pathway is activated by gluta minergic projections from the sensorimotor cortex and by dopaminergic nigral (pars compacta)-striatal projections. Activation of this direct pathway inhibits the medial pal lidum, which, in turn, disinhibits the ventrolateral and ventroanterior nuclei of the thalamus.