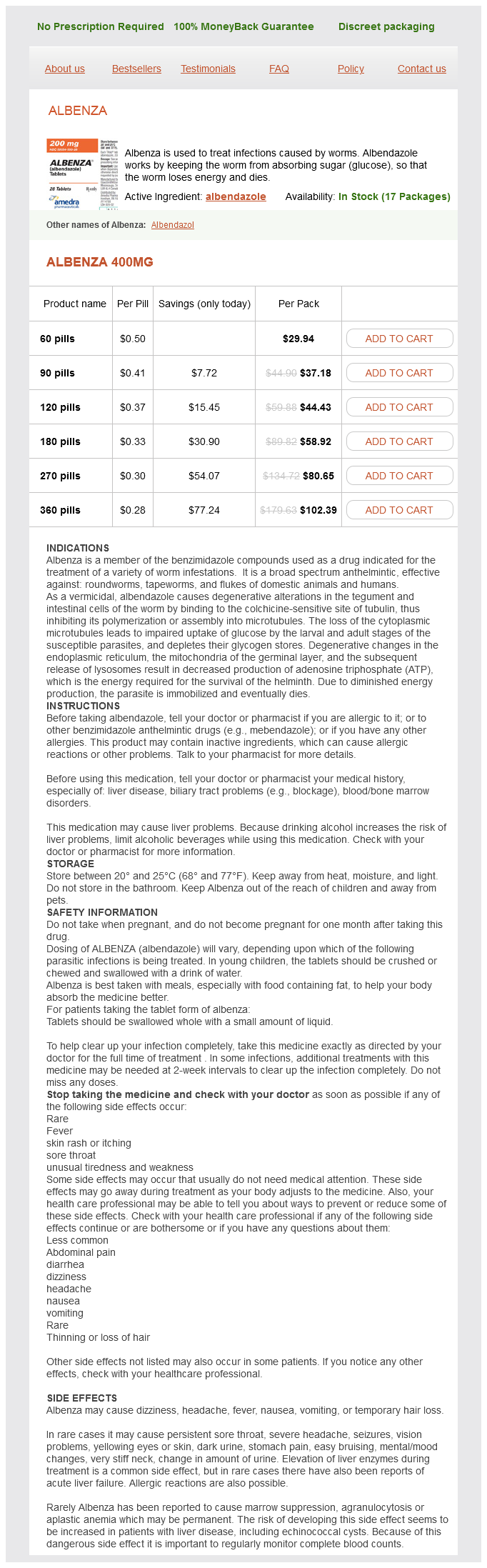
Albenza dosages: 400 mg
Albenza packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Cheap 400 mg albenza visa
When monetary abuse is sus pected, clinicians should pay consideration to the reporting require ments of their native jurisdictions. Patients with very mild or mild dementia based on the Clinical Dementia Rating Scale were in a position to cross formal highway checks at rates of 88% and 69%, respectively. Experts agree that patients with reasonably extreme or more advanced dementia must be recommended to stop driving. Although not nicely studied, clinicians should also contemplate the results of comorbid circumstances and medi cations and the function each may play in contributing to the chance of driving by a affected person with dementia. Finally, in some cases of delicate dementia, referral may be wanted to a driver rehabilitation specialist for analysis. Although not standardized, this evaluation often consists of both off- and on-road testing. Experts recommend such an evaluation for patients with gentle dementia, for these with dementia for whom new impairment in driving skills is observed, and for these with important deficits in cogni tive domains, corresponding to attention, govt function, and visuospatial abilities. Clinicians should additionally be conscious of the reporting require ments of their particular person jurisdictions. Some states have obligatory reporting laws for clinicians, but in different states, the choice to report an unsafe driver with dementia is voluntary. When a clinician has made the decision to report an unsafe driver to the Department of Motor Vehi cles, she or he should contemplate the impression of a possible breach in confidentiality and should weigh and address, prematurely when potential, the consequences of the loss of driving independence. Prog nosis Life expectancy after a diagnosis of Alzheimer illness is typically three - 1 5 years; it could be shorter than previously reported. Other neurodegenerative dementias, similar to dementia with Lewy bodies, present extra rapid decline. When to Refer Referral for neuropsychological testing could additionally be helpful to distinguish dementia from depression, to diagnose demen tia in individuals of very poor training or very excessive premor bid mind, and to help prognosis when impairment is mild. Screening for cognitive impairment in older adults: a systematic evaluation for the U. Advance Financial Planning Difficulty in managing monetary affairs usually develops early in the course of dementia. Other options to help in managing and monitoring finances embrace online banking, automatic bill funds, direct deposits, and j oint financial institution accounts. No gold-standard test is on the market to establish when a affected person with dementia not has monetary capacity. However, the clinician ought to be on the lookout for indicators that a affected person is both in danger for or actually experiencing monetary incapacity. Because financial impairment can happen when dementia is gentle, making that diagnosis ought to alone be enough to warrant additional investigation. Questioning sufferers and caregivers about late, missed, or repeated invoice payments, unusual or uncharacteristic 2. General Considerations Major depressive dysfunction occurs in as a lot as 5% of group dwelling older adults, whereas clinically vital depressive symptoms-often related to loss, illness, and life changes-are present in as a lot as 16% of older adults. Older patients with melancholy usually have a tendency to have somatic complaints, much less prone to report depressed mood, and more prone to expertise psychotic features than younger sufferers. Depressed elders could do higher with a collaborative or multidisciplinary care model that features socialization and other help components than with usual care. Clin ical Findings A simple two-question screen-which consists of asking "During the past 2 weeks, have you ever felt down, depressed, or hopeless Elderly patients with depressive signs ought to be questioned about use of alcohol and medicines (eg, ben zodiazepines, corticosteroids), since these might contribute to the medical image. Similarly, many medical issues could cause fatigue, lethargy, or hypoactive delirium, all of which can be mistaken for despair. Citalopram, methylphenidate, or their combi nation in geriatric despair: a randomized, double-blind, placebo controlled trial. Comparative efficacy and safety of selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors in older adults: a network meta-analysis. Treatment Treatment may involve psychosocial interventions, elevated physical activity, problem-solving remedy, cog nitive-behavioral therapy, discount of alcohol or medica tion intake, antidepressant medications, or a combination method. Choice of antidepressant agent is often based mostly on side-effect profile, value, and patient -specific factors, similar to presenting signs and comorbidities.
Buy albenza 400 mg on-line
General Considerations the superficial femoral artery is the peripheral artery mostly occluded by atherosclerosis. The illness fre quently happens where the superficial femoral artery passes by way of the abductor magnus tendon within the distal thigh (Hunter canal). The widespread femoral artery and the pop liteal artery are less generally diseased however lesions in these vessels are debilitating, resulting in short- distance claudication. Prognosis Patients with isolated aortoiliac illness might have an additional reduction in strolling distance with out intervention, but signs rarely progress to relaxation pain or threatened limb loss. Life expectancy is proscribed by their attendant cardiac illness with a mortality price of 25-40% at 5 years. Endovascular patency charges and symp tom aid for sufferers with quick stenoses are additionally good with 20% symptom return at three years. Recurrence charges fol lowing endovascular treatment of extensive illness are 30-50%. Symptoms and Signs Symptoms of intermittent claudication brought on by lesions of the frequent femoral artery, superficial femoral artery, and popliteal artery are confined to the calf. Paclitaxel eluting stents or paclitaxel-coated balloons supply modest improvement over bare steel stents and noncoated bal loons. The 1 -year patency price is 50% for balloon angio plasty, 70% for drug-coated balloons, and 80% for stents. It is far harder, nevertheless, to deal with restenosis in stents than vessels which have undergone angioplasty. Thromboendarterectomy-Removal of the atheroscle rotic plaque is proscribed to the lesions of the widespread femo ral and the profunda femoris arteries where bypass grafts and endovascular methods have a more limited role. However, with concomitant disease of the pro funda femoris or the popliteal artery, a lot shorter dis tances might trigger symptoms. With short-distance claudication, dependent rubor of the foot with blanching on elevation may be current. Chronic low blood flow states may even trigger atrophic changes in the lower leg and foot with lack of hair, thinning of the pores and skin and subcutaneous tissues, and disuse atrophy of the muscle tissue. With segmental occlusive illness of the superficial femoral artery, the com mon femoral pulsation is normal, but the popliteal and pedal pulses are decreased. In such sufferers, the toe brachial index is usually dependable with a value less than 0. Pulse volume recordings with cuffs placed on the excessive thigh, mid-thigh, calf, and ankle will delineate the levels of obstruction with reduced pressures and blunted waveforms. Myocardial infarction rates after open surgical procedure are 5 - 1 0%, with a 1 -4% mortality fee. Complica tion rates of endovascular surgery are 1 -5%, making these therapies engaging regardless of their lower durability. However, when claudication considerably limits day by day activity and undermines high quality of life in addition to over all cardiovascular health, intervention could additionally be warranted. All interventions require shut postprocedure follow-up with repeated ultrasound surveillance so that any recurrent narrowing could be treated promptly to stop full occlusion. The reported patency rate of bypass grafts of the femoral artery, superficial femoral artery, and popliteal artery is 65-70% at three years, whereas the patency of angio plasty is lower than 50% at three years. B ecause of the in depth atherosclerotic disease, includ ing related coronary lesions, 5-year mortality amongst sufferers with lower extremity disease could be as high as 50%, significantly with involvement of the infrapopliteal vessels. However, with aggressive danger factor modification, substantial improvement in longevity has been reported. Conservative Care As with aortoiliac disease, threat factor discount, medical optimization, and exercise treatment are the cornerstone of remedy. Revascularization is reserved for patients who stay significantly disabled after failure of this conserva tive routine. Bypass surgery-Intervention is indicated if claudication is progressive, incapacitating, or interferes significantly with important daily actions or employment. The best and sturdy treatment for lesions of the superficial femoral artery is a femoral-popliteal bypass with autogenous saphenous vein.
Order cheap albenza line
Treatment with inhaled beta- adrenergic agonists or intra venous aminophylline may be useful, however both can also provoke tachycardia and supraventricular arrhythmias. When the patient has improved, the cause or pre cipitating issue should be ascertained. In sufferers without prior heart failure, analysis should include echocardiog raphy and, in many cases, cardiac catheterization and coro nary angiography. Patients with acute decompensation of chronic coronary heart failure must be treated to achieve a euvolemic state and have their medical regimen optimized. In selected patients, early but cautious initiation of beta-blockers in low doses ought to be thought of. Less extreme decompensations normally present with dyspnea at relaxation, rales, and different evidence of fluid retention however with out extreme hypoxia. Noncardiac causes of pulmonary edema include intra venous opioids, elevated intracerebral strain, excessive alti tude, sepsis, medicines, inhaled toxins, transfusion reactions, shock, and disseminated intravascular coagula tion. These are distinguished from cardiogenic pulmonary edema by the scientific setting, history, and physical exami nation. The chest radiograph reveals signs of pulmonary vascu lar redistribution, blurriness of vascular outlines, increased interstitial markings, and, characteristically, the butterfly pattern of distribution of alveolar edema. The heart may be enlarged or regular in measurement relying on whether coronary heart fail ure was beforehand current. Treatment In full-blown pulmonary edema, the affected person must be placed in a sitting place with legs dangling over the facet of the bed; this facilitates respiration and reduces venous return. Noninvasive strain support ventilation might enhance oxygenation and stop severe C0 2 retention whereas pharmacologic interventions take effect. However, if respiratory distress remains severe, endotracheal intubation and mechanical ventilation could also be essential. Morphine is extremely effective in pulmonary edema and could additionally be helpful in much less severe decompensations when the affected person is uncomfortable. The initial dosage is 2-8 mg intravenously (subcutaneous administration is efficient in milder cases) and could also be repeated after 2-4 hours. It must be avoided in patients with opioid-induced pulmonary edema, who might enhance with opioid antagonists, and in these with neuro genic pulmonary edema. Intravenous diuretic therapy (furosemide, 40 mg, or bumetanide, 1 mg-or higher doses if the affected person has been receiving long-term diuretic therapy) is normally indicated even if the patient has not exhibited prior fluid retention. May present with chest pai n (pleuritic or nonspe cific) or signs of heart failure. Myoca rd ial biopsy, though not sensitive, might reveal a characteristic i nflammatory pattern. General Considerations Cardiac dysfunction because of major myocarditis is pre sumedly brought on by both an acute viral infection or a postviral immune response. Secondary myocarditis is the results of inflammation attributable to nonviral pathogens, medications, chemical substances, physical agents, or inflammatory diseases (such as systemic lupus erythematosus). The record of both infectious and noninfectious causes of myocarditis is intensive (Table 1 zero - 1 7. Both cellular and humoral inflammatory processes contribute to the professional gression to persistent injury, and there are subgroups that may profit from immunosuppression. Autoimmune myocarditis (eg, big cell myocarditis) may happen with no identifiable viral infection. Symptoms and Signs Patients may present a number of days to a couple of weeks after the onset of an acute febrile illness or a respiratory an infection or they may present with heart failure with out antecedent signs. Exam ination reveals tachycardia, a gallop rhythm, and other evi dence of coronary heart failure or conduction defects. Many acute infections are subclinical, although they may current later as idiopathic cardiomyopathy or with ventricular arrhythmias. Microaneurysms may occur and may be related to critical ventricular arrhythmias. Patients could current in a selection of methods with fulminant, subacute, or persistent myocarditis. In the European Study of Epidemiology and Treatment of Inflammatory Heart Disease, 72% had dys pnea, 32% had chest ache, and 1 8% had arrhythmias. The presence of Q waves or left bundle department block portends a better rate of demise or cardiac transplantation.

Albenza 400mg otc
Opioid Adverse Effects As opioids are titrated upward, growing difficulty with the unwanted aspect effects can be anticipated. Sedation may be expected with opioids, although toler ance to this effect and to unwanted effects other than constipa tion usually develops inside 24-72 hours at a stable dose. Opioid-induced neurotoxicity-including myoclonus, hyperalgesia, delirium with hallucinosis, and seizures-may develop in sufferers who take excessive doses of opioids for a protracted interval. Opioid-induced hyperalgesia appears to be a result of adjustments in both the peripheral and central nervous systems resulting in sensitivity to pain. Typically benign and even soothing stimuli (eg, mild massage) may be perceived as painful (allodynia), and growing opioid dose might exacerbate the problem. While ready for the level of the offending opioid to fall, low doses of lorazepam, baclofen, or gabapentin could also be helpful for treating myoclonus; halo peridol may be helpful for treating delirium. Avoiding or correcting dehydration could also be helpful for prevention and remedy of opioid-induced neurotoxicity. Notably, unrelieved constipation could also be a more likely cause of nausea within the setting of opioid use than opioid-induced nausea. Severe or persistent nausea despite remedy of constipation can be managed by switching opioids or by giving haloperidol, 0. Ondansetron, 4-8 mg orally or intravenously each 6 hours, also relieves nausea but can contribute to constipa tion. Mirtazapine and medical cannabis might every have a task in treating opioid-induced nausea. Although clinicians may worry about respiratory melancholy with opioids, this aspect impact is uncommon when a low dose is given initially and titrated upward slowly. Patients at explicit risk for respiratory melancholy include those with chronic obstructive pulmonary illness, obstructive sleep apnea, and baseline C0 2 retention; these with liver or kidney or combined liver-kidney failure; and those with adrenal insufficiency or frank myxedema. Yet, even sufferers with severe pulmonary disease and obstruc tive sleep apnea can tolerate low-dose opioids, however they should be monitored rigorously. Such a history suggests neuropathic ache, which is handled with some medications not typically used for different types of pain. While opioids are efficient for neuropathic pain, a selection of nonopioid drugs also have been found to be effective in randomized trials (Table 5-4). Successful management of neuropathic ache usually requires using a couple of effective treatment. Nortriptyline and desipramine are preferred as a result of they cause much less orthostatic hypotension and have fewer anticholinergic effects than amitriptyline. Start with a low dosage (1 0-25 mg orally daily) and titrate upward in 1 0-mg increments every four or 5 days aiming to use the low est efficient dose and titrating up to 100 mg day by day. Low-dose intravenous, oral, and nasal ketamine has been used successfully for neuropathic and different ache syndromes refractory to opi oids, though analysis knowledge are restricted. The calcium channel alpha2-delta ligands gabapentin and pregabalin are additionally first -line therapies for neuropathic ache. Gabapentin ought to be began at low dosages of 1 00-300 mg orally three times a day and titrated upward by 300 mg/day every four or 5 days with a typical efficient dose of 1 800-3600 mg/day. If needed, the dose of pregabalin may be titrated upward to 300-600 mg/day in two or three divided doses. Prescribing each gabapentin and an opioid for neuropathic pain may provide better analgesia at lower doses than if each is used as a single agent. Patients ought to be advised to take duloxetine on a full stomach as a result of nau sea is a typical aspect impact. Duloxetine may provide increased profit for neuropathic ache up to a total day by day dose of 120 mg, beyond the 60 mg restrict used for depres sion. Other medications efficient for neuropathic ache include tramadol, tapentadol, and the 5% lidocaine patch. The 5% lidocaine patch is effective in postherpetic neural gia and could additionally be efficient in other types of localized neuro pathic ache that causes hypesthesia. Hydrocodone has been probably the most commonly prescribed medication in the United States since no less than 2008, and the United States consumes 99% of the global provide. The whole amount of opioid prescriptions stuffed in 2007 would have been sufficient for each adult within the United States to receive 700 mg of morphine.
Order line albenza
Benzodiazepines may be efficient in preventing the anticipatory nausea related to chemotherapy. There is strong evidence that olanzapine may be effective for chemo therapy-induced nausea and vomiting. Careful consideration to affected person safety and nonpharmaco logic strategies to assist the affected person remain oriented (clocks, calendars, a familiar surroundings, reassurance and redi rection from caregivers) may be adequate to stop or handle gentle delirium. More generally, nonetheless, delirium on the finish of life is distressing to patients and family and requires therapy. While there are numerous reversible causes of delirium (see Chapter 25), figuring out and correcting the underlying trigger at the end of life is commonly complicated as a outcome of a patient could have many potential causes. The benefits of neuroleptic brokers within the therapy of agitation must be weighed care absolutely against potential harms, primarily based on proof showing an affiliation between antipsychotic drugs and increased mortality for older adults with dementia. Ramelteon, a melatonin agonist, at eight mg/ day orally has been proven to forestall delirium in significantly unwell, older hospitalized sufferers. When delirium is refractory to remedy and remains intolerable, sedation may be required to provide reduction and may be achieved quickly with mid azolam (0. Clinicians also can ask themselves "Would I be shocked if this patient died within the next yr Recognizing that patients might have completely different levels of comfort with prognostic data, clinicians can introduce the subject by simply saying, "I have details about the probably time course of your sickness. Parenteral hydration in patients with advanced most cancers: a multicenter, double-blind, placebo-controlled ran domized trial. Laxatives or methylnaltrexone for the manage ment of constipation in palliative care sufferers. Preventive results of ramelteon on delirium: a randomized placebo-controlled trial. The effect of methylphenidate on fatigue in superior cancer: an aggregated N -of- 1 Trial. Modafinil for the therapy of fatigue in lung cancer: outcomes of a placebo-controlled, double-blind, ran domized trial. Randomized, double-blind, placebo-controlled trial of oral docusate in the administration of constipation in hospice patients. Expectations About the End of Life Death is commonly regarded by clinicians, sufferers, and families as a failure of medical science. This angle can create or heighten a sense of guilt concerning the failure to forestall dying. B oth most people and clinicians typically are complicit in denying dying, treating dying persons merely as sufferers and dying as an enemy to be battled furiously in hospitals somewhat than as an inevitable consequence to be experienced as a part of life at home. As a end result, roughly 75-80% of individuals in the United States die in hospitals or long-term care facilities. Even when the clinician and patient continue to pursue remedy of potentially reversible illness, relieving suffering, offering help, and helping the affected person put together for demise must be foremost concerns. Patients on the end of life and their households determine a quantity of elements as essential to high quality end-of-life care: managing ache and different symptoms adequately, avoiding inappropriate pro longation of dying, communicating clearly, preserving dignity, making ready for demise, achieving a way of control, relieving the burden on others, and strengthening relation ships with loved ones. Caring for sufferers at the finish of life is a vital accountability and a rewarding opportunity for clinicians. From the medical perspective, the end of life may be defined as that point when death-whether because of terminal sickness or acute or continual illness-is expected inside weeks to months and may no longer be fairly fore stalled by medical intervention. Palliative care on the finish of life focuses on relieving distressing symptoms and promot ing high quality of life (as with all different phases of illness). For patients at the end of life, palliative care might become the only focus of care. Higher-quality communication is associated with higher satisfaction and consciousness of patient wishes. Clini cians should turn out to be proficient at delivering critical information and then coping with its consequences (Table 5-5). Smart phone and Internet communication sources can be found to assist clinicians, and preliminary evidence means that communication checklists may be effective. First, he or she should work to identify, understand, and relieve bodily, psychological, social, and spiritual distress or suffering. Patients require help for distress that will accompany discus sions of prognostic data.
Discount albenza 400 mg free shipping
The efficacy of combined inhaled corticosteroid and long performing beta-2-agonist therapy has led to the marketing of combination medicines that ship both brokers simulta neously (Table 9-3). At therapeutic doses, potential opposed effects embrace insom nia, aggravation of dyspepsia and gastroesophageal reflux, and urination difficulties in males with prostatic hyperpla sia. Dose-related toxicities include nausea, vomiting, tachyarrhythmias, headache, seizures, hyperglycemia, and hypokalemia. Leukotriene modifiers-Leukotrienes are potent bio chemical mediators that contribute to airway obstruction and asthma signs by contracting airway easy muscle, growing vascular permeability and mucus secre tion, and attracting and activating airway inflammatory cells. Zileuton is a 5-lipoxygenase inhibitor that decreases leukotriene manufacturing, and zafirlukast and montelukast are cysteinyl leukotriene receptor antagonists. These brokers are alternate options to low-dose inhaled corticosteroids in patients with delicate persistent bronchial asthma, although, as monotherapy, their impact is usually lower than inhaled corticosteroids. In real-life group trials, leu kotriene receptor antagonists have been equal in efficacy to an inhaled corticosteroid as first-line long-term controller medicine or to a long-acting beta-2-agonist as add-on therapy. Studies show a discount in bronchial asthma signs in sufferers treated with single-allergen immunotherapy. B ecause of the risk of immunotherapy induced bronchoconstriction, it ought to be administered solely in a setting the place such complications could be immedi ately handled. Omalizumab and reslizumab-Omalizumab is a recombinant antibody that binds IgE with out activating mast cells. In clinical trials in patients with moderate to severe asthma and elevated IgE levels, omalizumab reduced the necessity for corticosteroids. Vaccination-Patients with bronchial asthma should receive pneu mococcal vaccination (Pneumovax) and annual influenza (both seasonal and epidemic influenza A [H 1 N 1]) vaccina tions. Inactive vaccines (Pneumovax) are associated with few unwanted aspect effects, but the use of the reside attenuated influenza vaccine intranasally could also be related to asthma exacer bations in young children. The ophylline additionally has anti-inflammatory and immunomodula tory properties, enhances mucociliary clearance, and strengthens diaphragmatic contractility. Sustained-release theophylline preparations are efficient in controlling noc turnal signs and as added therapy in sufferers with average or severe persistent asthma whose symptoms are inadequately controlled by inhaled corticosteroids. When added to inhaled corticosteroids, theophylline might enable equivalent control at lower corticosteroid doses. These medications speed the resolu tion of airflow obstruction and scale back the rate of relapse. Delays in administering corticosteroids might lead to delayed benefits from these important brokers. Therefore, oral corti costeroids ought to typically be prescribed for early admin istration at house in sufferers with reasonable to extreme asthma. The minimal effective dose of systemic corticoste roids for asthma sufferers has not been recognized. It could additionally be prudent to administer corticosteroids intravenously to critically unwell patients to avoid concerns about altered gastrointestinal absorption. Antimicrobials-Multiple studies suggest that infections with viruses (rhinovirus) and bacteria (Mycoplasma pneu moniae, Chlamydophila pneumoniae) predispose to acute exacerbations of bronchial asthma and should underlie chronic, severe asthma. Quick-Relief Medications Short-acting bronchodilators and systemic corticosteroids are the necessary quick-relief drugs (Table 9-5). Beta-adrenergic agonists-Short-acting inhaled beta2-agonists, together with albuterol, levalbuterol, bitolterol, pir buterol, and terbutaline, are the most effective bronchodilators throughout exacerbations. All sufferers with acute symptoms ought to have immediate entry to considered one of these brokers. Beta-2-agonists chill out airway easy muscle and cause a prompt increase in air circulate and decrease in signs. Administration before exercise successfully prevents exercise-induced bronchocon striction. Inhaled beta-adrenergic remedy is as efficient as oral or parenteral therapy in stress-free airway smooth muscle and improving acute asthma and provides the benefits of speedy onset of action (less than 5 minutes) with fewer systemic unwanted facet effects. With most beta-2-agonists, the beneficial dose by nebulizer for acute asthma (alb utero! Increased use (more than one canister a month) or lack of anticipated impact indicates diminished asthma management and the necessity for additional long-term con trol therapy. Anticholinergics-Anticholinergic agents reverse vagally mediated bronchospasm but not allergen- or exercise induced bronchospasm. Adjustments to that algorithm comply with a stepwise method based mostly on a cautious assessment of bronchial asthma management.
Albenza 400mg on line
Traditional endpoints of resuscitation corresponding to blood stress, heart price, urinary output, psychological standing, and skin perfusion can therefore be deceptive. At doses of 5 - 1 0 meg/kg/min, beta- 1 -adrenergic effects predominate, leading to an increase in heart price and cardiac contractility. At higher doses (greater than 10 meg/ kg/min), alpha-adrenergic results predominate, resulting in peripheral vasoconstriction. Norepinephrine is the initial vasopressor of selection in septic shock to maintain the imply arterial pres sure at 65 mm Hg or higher. In meta-analyses, the use of dopamine as a first-line vasopressor in septic shock resulted in a rise in 28-day mortality and a higher incidence of arrhythmic events. Dopamine should only be used as an alternative to norepinephrine in choose patients with septic shock, together with patients with vital bra dycardia or low potential for tachyarrhythmias. The rationale for utilizing low-dose vaso pressin within the administration of septic shock consists of the relative deficiency of vasopressin in late shock. Vasopressin additionally potentiates the results of catecholamines on the vascu lature and stimulates cortisol production. Some studies have reported decreased catecholamine requirements with vasopressin administration. Higher doses of vasopressin decrease cardiac output and may put sufferers at higher threat for splanchnic and coronary artery ischemia. There is inadequate proof to recommend a particular vasopressor to use in cardiogenic shock, but professional opinion suggests that either norepinephrine or dopamine be used as a first-line agent. Dobutamine, a predominantly beta adrenergic agonist, will increase contractility and decreases afterload. Tachyphy laxis can occur after 48 hours secondary to the down-regulation of beta-adrenergic receptors. Amrinone and milrinone are phosphodiesterase inhibitors that could be substituted for dobutamine. Antibiotics-Definitive therapy for septic shock consists of early initiation of empiric broad-spectrum antibiotics after appropriate cultures have been obtained and within 1 hour of recognition of septic shock. Surgi cal administration may be necessary if necrotic tissue or loculated infections are present (see Table 30-5). Other Treatment Modalities Cardiac failure may require use of transcutaneous or trans venous pacing or placement of an intra-arterial balloon pump. Emergent revascularization by percutaneous angio plasty or coronary artery bypass surgery seems to enhance long-term outcome with elevated survival compared with initial medical stabilization for sufferers with myocardial ischemia resulting in cardiogenic shock. Urgent hemodialy sis or continuous venovenous hemofiltration could additionally be indi cated for maintenance of fluid and electrolyte stability throughout acute kidney damage leading to shock from multi ple modalities. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 20 1 2. Poor food plan could lead to folic acid deficiency and contribute to iron deficiency, but bleeding is the most common reason for iron deficiency in adults. Attention to bodily signs of major hematologic diseases (lymphadenopathy; hepatosplenomegaly; or bone tenderness, particularly in the sternum or anterior tibia) is essential. Anemias are categorised in accordance with their pathophysio logic foundation, ie, whether or not related to diminished manufacturing (relative or absolute reticulocytopenia) or to elevated production due to accelerated loss of pink blood cells (retic ulocytosis) (Table 1 three - 1), and according to red blood cell size (Table 13-2). A reticulocytosis happens in certainly one of three pathophysiologic states: acute blood loss, latest replace ment of a lacking erythropoietic nutrient, or lowered red blood cell survival (ie, hemolysis). A bone marrow biopsy is generally needed to full the evaluation of anemia when the laboratory evaluation fails to reveal an etiology, when there are extra cytopenias current, or when an underlying primary or secondary bone marrow process is suspected. General Considerations Iron deficiency is the most common reason for anemia worldwide. Aside from circulating purple blood cells, the major location of iron in the body is the storage pool as ferritin or as hemosiderin in macrophages. About 10% of this amount is absorbed within the stom ach, duodenum, and higher j ejunum under acidic condi tions. Dietary iron present as heme is efficiently absorbed (1 0-20%) but nonheme iron much less so (1 -5%), largely due to interference by phosphates, tannins, and different meals constituents. The main iron transporter from the food regimen across the intestinal lumen is ferroportin, which additionally facili tates the transport of iron to apotransferrin in macro phages for delivery to erythroid cells ready to synthesize hemoglobin. Hepcidin, which is more and more produced throughout inflammation, negatively regulates iron transport by promoting the degradation of ferroportin. Small amounts of iron-approximately 1 mg/day-are usually misplaced by way of exfoliation of pores and skin and mucosal cells.
Generic albenza 400mg overnight delivery
Compensatory vasoconstriction might transiently maintain the blood stress however unreplaced losses of over 1 5 % of the intravascular volume can outcome in hypotension and progressive tissue hypoxia. The reduction in systemic vascular resistance leads to insufficient cardiac output and tissue hypo perfusion regardless of regular circulatory quantity. Loss of bl ood (hemorrhagic sh ock) External hemorrhage Tra uma Gastroi ntestinal tract bleeding I nternal hemorrhage Hematoma Hemothorax or hemoperitoneum Loss of plasma Burns Exfoliative dermatitis Loss of fl uid and electrolytes External l osses Vomiting Dia rrhea Excessive sweating Hyperosmolar states (dia betic ketoacidosis, hyperosmolar non ketotic coma) I nternal losses (th i rd spacing) Pa ncreatitis Ascites Bowel obstruction Cardiogenic shock 1. Septic shock-Sepsis is the most typical explanation for dis tributive shock and carries a mortality rate of 20-50%. Sepsis is outlined as the presence of infection (either documented or suspected) in conjunction with systemic manifestations of an infection. Septic shock is diagnosed when hypotension from sepsis persists despite adequate fluid resuscitation. The most typical reason for septic shock in hospitalized sufferers is an infection with gram-positive or gram-negative organisms, with a rising incidence of infection from multidrug resistant organisms. Sepsis from fungal organisms is increas ing but remains lower than that for bacterial infections. Risk components for septic shock embody bacteremia, extremes of age, diabetes, most cancers, immunosuppression, and history of a latest invasive process. Neurogenic shock-Neurogenic shock is brought on by traumatic spinal wire injury or effects of an epidural or spinal anesthetic. This leads to lack of sympathetic tone with a reduction in systemic vascular resistance and hypo rigidity and not utilizing a compensatory tachycardia. Reflex vagal parasympathetic stimulation evoked by ache, gastric dila tion, or fright could simulate neurogenic shock, producing hypotension, bradycardia, and syncope. The clinical definition of cardiogenic shock is evidence of tissue hypoxia as a outcome of decreased cardiac output (cardiac index lower than 2. This is most frequently caused by myocardial infarction however can additionally be because of cardiomy opathy, myocardial contusion, valvular incompetence or stenosis, or arrhythmias. A drop in systolic pressure of larger than 1 0-20 mm Hg or an increase in pulse of greater than 1 5 beats per minute with positional change suggests depleted intravascular quantity. However, blood strain is commonly not the most effective indicator of end-organ perfusion as a end result of compensatory mechanisms, such as elevated coronary heart fee, increased cardiac contractility, and C. Obstructive Shock Cardiac tamponade, tension pneumothorax, and large pulmonary embolism may cause an acute lower in car diac output leading to shock. Patients with hypotension usually have cool or mottled extremities and weak or thready peripheral pulses. Splanch nic vasoconstriction could lead to oliguria, bowel ischemia, and hepatic dysfunction, which may ultimately lead to multi-organ failure. Mentation could also be regular or patients might turn into stressed, agitated, confused, torpid, or comatose on account of insufficient perfusion of the mind. Hypovolemic shock is evident when signs of hypoper fusion, corresponding to oliguria, altered psychological standing, and cool extremities, are present. In cardiogenic shock, there are additionally indicators of global hypoperfusion with oliguria, altered mental status, and funky extremities. Jugular venous strain is elevated and there may be proof of pulmonary edema with respiratory compromise in the setting of left-sided coronary heart failure. In hypovo lemic shock, the left ventricle shall be small because of decreased filling, but contractility is commonly preserved. Car diogenic shock outcomes from cardiac failure with a resultant lower in left ventricular contractility. In some cases, the left ventricle could appear dilated and full because of the lack of the left ventricle to ej ect a adequate stroke volume. In distributive shock, indicators include hyperdynamic heart sounds, heat extremities initially, and a large pulse pressure indicative oflarge stroke quantity. Fluid resus citation might have little effect on blood stress, urinary output, or mentation.