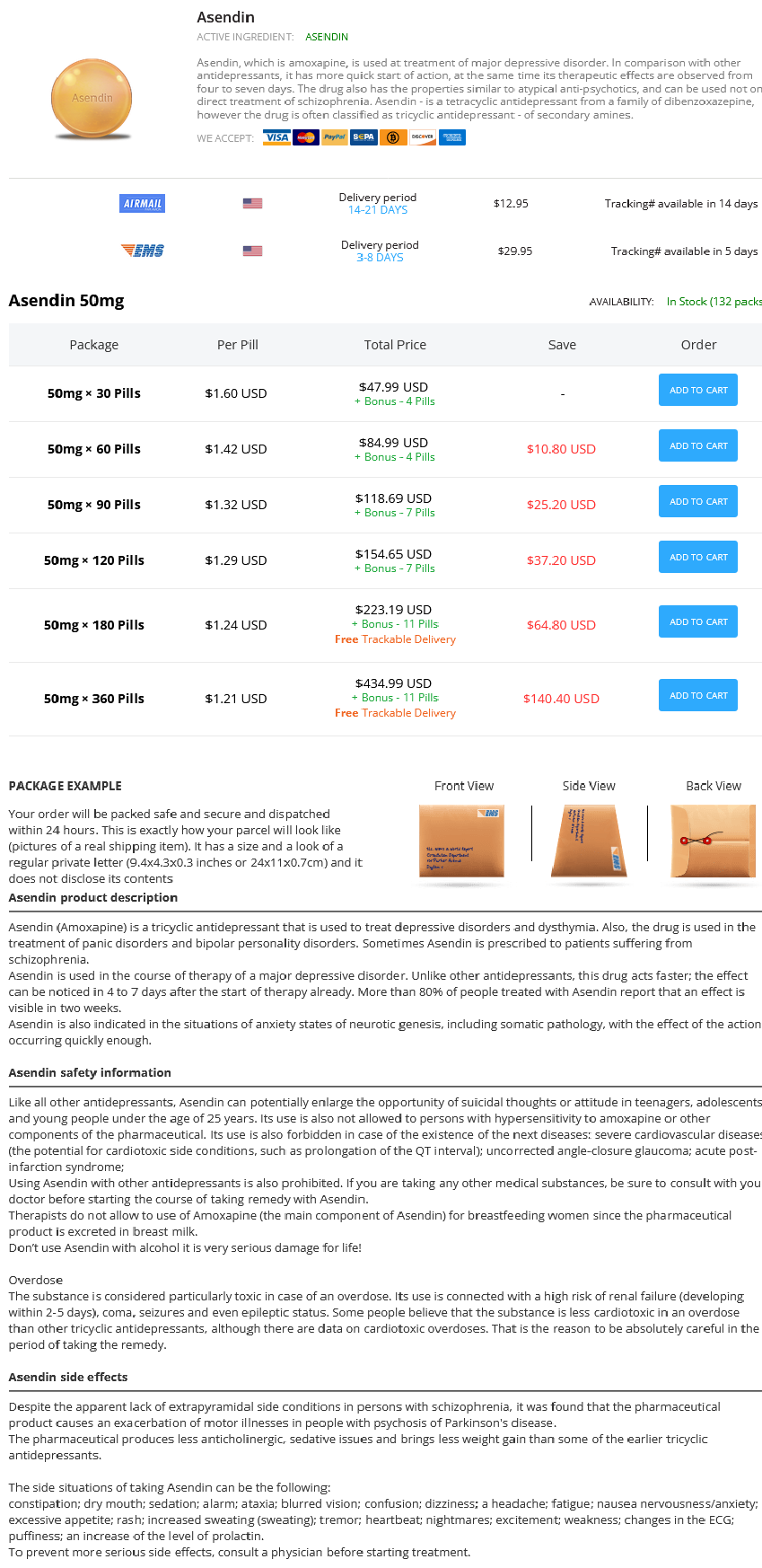
Asendin dosages: 50 mg
Asendin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Discount asendin 50 mg otc
Resection is similar to resection in the knee as a ligamentum mucosa may be excised leaving the anterior cruciate ligament alone. The spinoglenoid ligament laterally resected will go away the nerve seen heading medially untouched. The ligament may be followed to the glenohumeral joint at its insertion to understand and visualize safely the entire resection of the ligament. By staying on the spine of the scapula during resection, bleeding shall be minimized. The shaver is taking the spinoglenoid ligament directly off the spine of the scapula. Arthroscopic view of the left shoulder, posterior view, with the arrow pointing to the suprascapular nerve heading medially. Note the bulging tissue to the left, representing a ganglion cyst not yet decompressed. Postoperative Protocol Rehabilitation is affected by any extra procedures performed at the aspect of the suprascapular nerve release. Patients are instructed in the usage of a sling for consolation for the primary postoperative week routinely. For isolated suprascapular nerve releases, sufferers are seen in the workplace postoperative day 1, and pendulum exercises and progressive range of movement exercises are initiated. Patients are then permitted to enhance their exercise as tolerated with return to full overhead activities within 6 weeks. A full therapy strengthening program can start at 6 weeks if a suprascapular nerve decompression is the one process performed on the shoulder. The ability to restore muscle power and reverse the muscle atrophy may be very tough if not impossible. Patients ought to be clearly informed of the limitation to not be capable of restore normal power previous to surgical procedure. When releasing the transverse scapular ligament, identification of the artery is at all times carried out to keep away from laceration. No sequence to date has reported any an infection postoperatively from either of those procedures. This approach is safe and efficient as a minimally invasive answer for suprascapular nerve entrapment. Accurately establish the floor landmarks and draw out with a ruler the precise location of all portals. Keep the systolic blood stress below a hundred mm Hg to enable for optimal visualization and the pump strain at a low setting (eg, forty five mm Hg) to avoid pointless swelling. Perform the discharge of the suprascapular nerve on the transverse scapular ligament and spinoglenoid ligament first, previous to any other further process, to guarantee swelling in the shoulder is kept to a minimal. Arthroscopic Suprascapular Nerve Release: the Transverse Scapular Ligament 231 References 1. Posterior shoulder pain: a dynamic study of the spinoglenoid ligament and therapy with arthroscopic launch of the scapular tunnel. The incidence of nerve damage in anterior dislocation of the shoulder and its influence on practical recovery. Suprascapular nerve entrapment by ganglion cysts: a report of six circumstances with arthroscopic findings and evaluate of the literature. Suprascapular entrapment neuropathy: a scientific, anatomical, and comparative examine. Posterior shoulder pain and arthroscopic decompression of the suprascapular nerve at the transverse scapular ligament. Arthroscopic decompression of the suprascapular nerve on the spinoglenoid notch and suprascapular notch by way of the subacromial area. Posterior shoulder ache and arthroscopic decompression of the suprascapular nerve on the spinoglenoid notch. Most subscapularis tears are discovered in older patients together with the anterosuperior tear sample in which the anterolateral supraspinatus tendon, biceps, and rotator interval are also concerned.
Fumus (Fumitory). Asendin.
- How does Fumitory work?
- Spasms of the gut, skin conditions, eye irritation, heart problems, bile (a fluid secreted from the liver) disorders, and other conditions.
- Are there safety concerns?
- Irritable bowel syndrome (IBS). Taking fumitory does not seem to improve symptoms of irritable bowel syndrome.
- Dosing considerations for Fumitory.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96460
Asendin 50 mg generic
If 90 g of glucose had been dissolved in 1 L of water, the solution would have a focus of 0. Thus, a 1 mol/L resolution of glucose incorporates the identical number of solute molecules per liter as a 1 mol/L resolution of any other substance. The concentrations of solutes dissolved within the physique fluids are a lot lower than 1 mol/L. By convention, the liter (L) term is typically dropped when referring to concentrations. Thus, a 1 mmol/L resolution is often written as 1 mM (the capital "M" stands for "molar" and is defined as mol/L). An instance of the importance of solute concentrations is said to a key homeostatic variable, that of the pH of the body fluids, as described next. Maintenance of a narrow vary of pH (that is, hydrogen ion concentration) in the physique fluids is completely important to most physiological processes, in part as a result of enzymes and other proteins depend upon pH for his or her normal form and exercise. The acidity of a solution thus refers to the free (unbound) hydrogen ion concentration in the resolution; the higher the hydrogen ion focus, the greater the acidity. The brackets around the image for the hydrogen ion in the following method point out focus: pH 5 2log [H1] Hydrogen Ions and Acidity As talked about earlier, a hydrogen atom consists of a single proton in its nucleus orbited by a single electron. The most typical sort of hydrogen ion (H1) is formed by the loss of the electron and is, due to this fact, a single free proton. Note that as the acidity increases, the pH decreases; a change in pH from 7 to 6 represents a 10-fold increase within the hydrogen ion focus. The extracellular fluid of the physique has a hydrogen ion concentration of about 4 3 1028 mol/L (pH 5 7. Most intracellular fluids have a slightly larger hydrogen ion concentration (pH 7. As we noticed earlier, the ionization of carboxyl and amino teams includes the release and uptake, respectively, of hydrogen ions. Also, notice that by conference, separate terms are used for the acid forms-lactic acid and carbonic acid-and the bases derived from the acids-lactate and bicarbonate. By combining with hydrogen ions, bases decrease the hydrogen ion focus of an answer. In the case of lactic acid, nonetheless, only a fraction of the lactic acid molecules in solution launch hydrogen ions at any prompt. Therefore, if a 1 mol/L answer of lactic acid is in contrast with a 1 mol/L answer of hydrochloric acid, the hydrogen ion focus shall be decrease within the lactic acid solution than within the hydrochloric acid solution. Hydrochloric acid and other For example, if the acidity of an answer containing lactate is increased by including hydrochloric acid, the concentration of lactic acid will enhance and that of lactate will lower. If the electrical cost on a molecule is altered, its interaction with other molecules or with other regions throughout the same molecule modifications, and thus its functional characteristics change. In the extracellular fluid, hydrogen ion concentrations past the 10-fold pH range of seven. Even small adjustments in the hydrogen ion focus can produce massive adjustments in molecular interplay. For instance, many enzymes within the body operate efficiently inside very slim ranges of pH. Should pH vary from the normal homeostatic vary as a outcome of disease, these enzymes work at lowered charges, creating a good worse pathological state of affairs. We flip now to a description of the natural molecules important for life in all living organisms, Chemical Composition of the Body and Its Relation to Physiology 29 together with humans. These are the carbon-based molecules required for forming the constructing blocks of cells, tissues, and organs; offering energy; and forming the genetic blueprints of all life. One of the properties of the carbon atom that makes life possible is its ability to kind four covalent bonds with other atoms, including with different carbon atoms. Because carbon atoms also can combine with hydrogen, oxygen, nitrogen, and sulfur atoms, an unlimited number of compounds can type from relatively few chemical parts. In some instances, such giant molecules kind when many similar smaller molecules, known as subunits or monomers (literally, "one half"), link together. The construction of any polymer relies upon upon the construction of the subunits, the number of subunits bonded together, and the three-dimensional means in which the subunits are linked. Most of the organic molecules within the body can be classified into certainly one of 4 groups: carbohydrates, lipids, proteins, and nucleic acids (Table 2.
Buy asendin 50 mg low price
With a bullet tip reamer, the surgeon drills a 20-mm deep bone socket roughly 10 mm above the pectoralis main tendon. Typically, a 9-mm diameter tunnel is drilled for feminine patients and a 10-mm diameter tunnel is drilled for male patients. Illustration indicating the related anatomy for an arthroscopic biceps tenodesis. Step 4: Restoring the Correct Length-Tension Relation A main objective of the tenodesis process is to restore the normal length-tension relation of the tendon. To obtain a normal length-tension relation, the buried phase must derive from the tendon proximal to the bone socket. By doing so, the authors stop steering of the distal tendon segment into the socket. Before tenotomy, the authors carry out a tag sew through the tendon exactly on the level of the cartilage rim. This surgical gesture holds the tendon after tenotomy and acts as a useful landmark for extra measurements. The mean tendon length from the extent of the cartilage rim as much as the superior border of the pectoralis major tendon is approximately 50 to 55 mm. Therefore, the distance between the bone socket and the holding sew is forty to 45 mm. A sizer can be used to take the measurements; however, any instrument can work for this task as a caliper. If the planned interference screw is 20-mm long, then the forked tip ought to grab the tendon 20 to 25 mm above the socket stage or roughly midway between the superior fringe of the pectoralis major tendon and the articular cartilage rim. Step 5: Tenotomy and Interference Screw Fixation After retrieving the sutures of the superior tag stitch from the posterior portal, tenotomy is performed with radiofrequency right earlier than interference screw fixation. There are a variety of techniques for biceps tenodesis in the market; nevertheless, all of them share the identical ideas. Some implants have a polyetheretherketone forked tip as part of the insert to push the tendon inside the socket. In other devices, the fork is a half of the instruments and it comes out before screw fixation. By loading the sutures tails through the eyelets on the implant tip, the surgeon can simply steer the tendon contained in the socket, obtaining an optimum length-tension relation. Use depth indicators on the distal end of the tendon fork to make certain the tendon is absolutely seated into the socket. A trocar tipped information wire is placed by way of the fork to hold the tendon into the socket. Strengthening and gradual return to sports activities are anticipated between three and 5 months after surgery. Due to intraoperative bleeding and visualization issues, the process might require conversion to an open subpectoral tenodesis. At medium-term scientific follow-up (mean 14 months, range 6 to 32 months), the authors observed fixation failure ("Popeye sign") in four instances (8. Furthermore, the open subpectoral tenodesis with distal fixation near a slender diaphysis has a higher threat of humeral fracture. To guarantee a pleasant surgical procedure, place the affected person in the beach chair place, use the scope by way of the lateral portal, and create 2 anterior portals for introduction of surgical tools. All of the dissections and tissue removal have to be accomplished with a radiofrequency gadget. Retract and maintain the tendon out of the groove with a switching stick and use the reamer in a exactly perpendicular fashion to the bone. Only steer into the socket tendon phase that originated proximally to the socket. Comparison of forearm supination and elbow flexion energy in patients with lengthy head of the biceps tenotomy or tenodesis. Outlet biceps tenodesis: a brand new approach for treatment of biceps lengthy head tendon damage. Minimally invasive proximal biceps tenodesis: an anatomical research for optimum placement and protected surgical method. Biomechanical efficiency of subpectoral biceps tenodesis: a comparability of interference screw fixation, cortical button fixation and interference screw diameter.
Discount asendin 50mg on-line
The (posterior) interscalene space is located bet ween the scalenus anterior and m edius and the rst rib and is traversed by the brachial plexus and subclavian artery. The subclavian vein passes deeply via the interval form ed by the scalenus anterior, the sternocleidom astoid m uscle (resected), and the rst rib (the anterior interscalene space). The principal arterial vessel on this area is the occipital artery, the second branch arising from the posterior facet of the exterior carotid artery. The m edially situated higher occipital nerve is a dorsal ram us of the C2 spinal nerve, while the laterally located lesser occipit al nerve is a ventral ram us of C2 that arises from the cervical plexus (see p. The lym ph nodes are located at the websites where the nerves and veins em erge by way of the cervical fascia. Note the accent nerve, which crosses the lat-eral cervical triangle at a comparatively super cial degree. Topographical Anatomy Occipital artery Splenius capitis Sternocleidom astoid Sem ispinalis capitis Obliquus capitis superior Rectus capitis posterior m inor Greater occipital nerve Vertebral artery Rectus capitis posterior m ajor Obliquus capitis inferior Spinous process, axis (C2) Third occipital nerve Sem ispinalis cervicis m uscle Splenius capitis Suboccipital nerve Occipital artery Great auricular nerve Transverse means of atlas (C1) Cervical posterior intertransversarius Longissim us capitis Sem ispinalis capitis B Right suboccipital triang le Posterior view. The suboccipital triangle is bounded superiorly by the rectus capitis posterior m ajor, laterally by the obliquus capitis superior, and inferiorly by the obliquus capitis inferior. This m uscular triangle may be seen only after the trapezius, splenius capitis, and sem ispinalis capitis m uscles have been rem oved. A brief, free segm ent of the vertebral artery runs by way of the deep a half of the triangle after leaving the transverse foram en and before exiting the triangle by perforating the atlanto-occipital m em brane (not visible here). That segm ent of the vertebral artery provides o branches to the encompassing quick nuchal m uscles. The examination iner take a look at s the feeling of those nerves by urgent flippantly on the circled level s with the thum b. If these point s (but not their surroundings) are painful, the nding is described, logically, as "tenderness over the occipital nerves. The pat tern of segm ental innervation is illustrated on the left, and the territorial assignm ents of speci c cutaneous nerves on the right. The occiput and neck derive m ost of their segm ental innervation from the second and third cervical segm ent s. Note that in the peripheral innervation pat tern, the higher occipitalnerve is a dorsal spinal nerve ram us while the lesser occipital nerve is a ventral ram us (see p. This section of the cranium may be roughly subdivided into four areas: the oral cavit y, the nasal cavit y and sinus, the orbit, and the anterior cranial fossa. Inspecting the area in and around the oral cavity, we observe the m uscles of the oral oor, the apex of the tongue, the neurovascular structures within the m andibular canal, and the rst m olar. The onerous palate separates the oral cavit y from the nasal cavity, which is split into left and proper halves by the nasal septum. The inferior and m iddle nasal conchae can be identi ed along with the laterally situated m axillary sinus. The part passes by way of the transparent vitreous body, and three of the six extraocular m uscles may be identi ed in the retro-orbital fat. Note: the bony orbital plate (m edial wall of the orbit) could be very skinny (lam ina papyracea) and m ay be penetrated by an infection, traum a, and neoplasm s. In the anterior cranial fossa, the part passes through each frontal lobes of the mind within the m ost anterior parts of the cerebral gray m at ter. In addition to the oral oor m uscles, we see the m uscles of m astication on the sides of the skull. The orbit com m unicates laterally with the infratemporal fossa through the inferior orbital ssure. This part cut s via both olfactory bulbs in the anterior cranial fossa, and the superior sagit tal sinus may be recognized within the m idline. The soft palate replaces the exhausting palate in this aircraft of part, and the nasal septum becom es osseous at this degree. This coronal part is slightly angled, producing an apparent discontinuit y within the m andibular ram us on the left facet of the gure (compare with the continual ram us on the proper side). Above the roof of the sphenoid sinuses is the hypophysis (pituitary), which lies in the hypophyseal fossa. In the cranial cavit y, the aircraft of part passes via the m iddle cranial fossa. Due to the presence of the carotid siphon (a 180� bend in the cavernous a part of the inner carotid artery), the part cut s the internal carotid artery t wice on both sides.
Generic asendin 50 mg fast delivery
By de nition, t wo form s of brachial plexus paralysis are distinguished: upper brachial plexus paralysis, which is brought on by a lesion of the C 5 and C 6 ventral ram i (see C), and lower brachial plexus paralysis, which is caused by a lesion of the C 8 and T 1 ventral ram i (see D). C 7 form s a "watershed" bet ween the t wo type s of paralysis and is t ypically una ected by both kind. Because the ventral ram i carry both m otor and sensory bers, a brachial plexus lesion all the time causes a com bination of m otor and sensory de cit s. The resulting paralysis (see C) is always of the accid t ype because of it s peripheral nature (lesion of the second m otor neuron). The arm hangs limply at the facet (loss of the upper arm exors), and the palm faces backward (loss of the supinator with dom inance of the pronators). There m ay also be partial paralysis of the extensor m uscles of the elbow joint and hand. Typical cases present with sensory disturbances on the lateral surface of the upper arm and forearm, however these signs m ay be absent. It a ect s the hand m uscles, the digital exors, and the exor m uscles within the wrist (claw hand with atrophy of hand m uscles, a). Because the sympathetic bers for the top go away the spinal wire at T 1 (b), the sympathetic innervation of the top can be misplaced. This is m anifested by a unilateral Horner syndrome, characterised by m iosis (contracted pupil as a outcome of paralysis of the dilator pupillae) and narrowing of the palpebral ssure (not ptosis) due to a loss of sympathetic innervation to the superior and inferior tarsal m uscles. The narrowed palpebral ssure m im ics enophthalm os (sinking of the eyeball into the orbit). The lum bosacral plexus is divided into a lum bar plexus (T 12�L4) and sacral plexus (L5�S 4). The inferior bers of L4 as nicely as all bers of L5 m erge to type the lum bosacral trunk, which is the connection to the sacral plexus. Note: Most nerves of the lum bar element run in ventral direction whereas the nerves from the sacral element run in dorsal course. Lesions to the lum bosacral plexus happen in case of fractures of the pelvis ring, sacrum or hip and as a outcome of hip replacem ent. The lesion also disrupts the sympathetic bers for the leg, which come up from the lumbar twine and cross via the lum bar plexus. The clinical manifestations (b) include increased heat of the foot (loss of sympathetic vasoconstriction) and anhidrosis on the sole of the foot (sweating is absent because of lack of sympathetic innervation to the sweat glands). When sweating is undamaged, the ninhydrin check is constructive (footprint on a sheet of paper stains purple with 1% ninhydrin solution). Note: Manifestations within the lim bs are acknowledged by comparability with the una ected aspect. The result s are loss of plantar exion (tibial nerve paralysis, inabilit y to stroll on the toes) and paralysis of the foot and toe extensors (com m on bular nerve, steppage gait: the patient m ust increase the knee abnorm ally excessive whereas strolling to keep away from dragging the toes on the ground). Sensory disturbances are noted on the posterior surfaces of the thigh, decrease leg, and foot. Because the superior gluteal nerve is concerned, the gluteus m edius and m inim us are additionally paralyzed. Speci c classes of peripheral nerve lesions are described in the volum e on General Anatomy and Musculoskeletal System. This is determ ined system atically by proceeding from the periphery of the twine towards the center. We will then focus on the extent of the lesion within the longitudinal or craniocaudal dim ension. Since these syndrom es present with de cits that end result from dam age to speci c anatom ical constructions, they can be explained in anatom ical term s. Based on the lesions and syndrom es described here, the reader can check his or her abilit y to relate what has already been realized to the areas and e ects of spinal wire lesions. A Spinal ganglion syndrome illustrated for an isolated lesion of T6 As part of the dorsal roots, the dorsal root (spinal) ganglia are involved with the transm ission of sensory inform ation. Because the derm atom es present considerable overlap, adjacent derm atom es can assum e the perform of the a ected derm atom. As a end result, the world that shows absolute sensory loss, referred to as the "autonom ous area" of the derm atom e, m ay be fairly sm all. When this sensory loss a ect s the a erent lim b of a re ex, that re ex might be absent or dim inished.
Cheap asendin 50mg line
The arm is then positioned at 30 to 40 degrees of abduction and 20 levels of ahead flexion. The authors choose to apply 10 lbs of each longitudinal and abduction pressure for balanced traction. One advantage of the lateral decubitus position is that it avoids issues with cerebral hypoperfusion which have been associated with the beach chair place and will discourage anesthesiologists from utilizing hypotensive anesthesia. The authors prefer to utilize each an ultrasound-guided interscalene or supraclavicular block and common anesthesia. Examination Under Anesthesia and Arthroscopic Evaluation of the Superior Labrum First, carry out an examination under anesthesia to doc passive vary of motion, anterior and posterior laxity, and the magnitude of the sulcus signal. A standard posterior arthroscopic portal ought to then be established 2 cm medial and 1 cm distal to the posterolateral acromion. An arthroscopic passive compression check or Mayo shear check can also be carried out to evaluate for superior labrum instability. Next, an anterior portal is created with an outside-in method within the rotator interval, slightly extra superior than during Bankart restore to facilitate the use of suture-passing devices. Insert a cannula giant sufficient to enable for supply of suture-passing devices. A probe launched into this portal can then be used to additional assess the superior labrum for stability in addition to to manipulate the bicep tendon to assess for lengthy head of biceps tendinopathy. At this juncture, the surgeon should additionally determine whether or not the superior labrum is pathologic or physiologic, processes that can be difficult to differentiate. Experience and data of the spectrum of anatomic variations within the superior and anterosuperior labrum are crucial. However, whatever the arthroscopic appearance, the surgical choice making is always based mostly on the arthroscopic findings within the context of the history and physical exam findings. Labral Preparation and Accessory Portal Placement Options the anterior cannula sometimes serves as the working cannula for labral preparation and the passing of sutures. To avoid causing iatrogenic chondral damage to the glenoid, the surgeon ought to begin the burr off of bone with the enamel dealing with barely medial. A cylindrical-shaped burr is typically easier to management in comparison with an acornshaped burr. Once the superior glenoid bone preparation is complete, the surgeon should create an accessory portal for anchor insertion and potential suture shuttling. A portal may be established at the superior side of the rotator interval simply off of the main edge of the supraspinatus to present anterosuperior and midanterior portals throughout the rotator interval. If 2 rotator interval portals are used, ensure that maximal distance separates the portals to keep away from crowding. The benefit of utilizing 2 cannulas inside the interval is that harm to the rotator cuff is minimized. While viewing from either the posterior or anterior portal, a spinal needle is used for localization. The trans-rotator cuff portal pores and skin incision is often just off of the lateral acromion simply posterior to the anterolateral nook. To carry out the knotless suture anchor fixation, the authors choose to insert a small 5-mm metallic cannula on this trans-rotator cuff portal to minimize rotator cuff damage. Care should be taken to make sure that this portal passes medial to the rotator cable. This portal lies 1 cm anterior and 1 cm lateral to the posterolateral corner of the acromion. Knotted Suture Anchor Fixation vs Knotless Suture Anchor Fixation the surgeon then has 2 choices for suture anchor labral fixation: a knotless or a knotted suture anchor approach. Passage of a shuttling suture by way of the chondrolabral junction from the anterosuperior portal (cannula can be seen behind the biceps). The suture shuttle handed from the anterior cannula through the labrum could be retrieved from the trans-cuff portal utilizing a suture-retrieving gadget. A broad free suture (Labral tape) is tied to the shuttling suture and delivered back beneath the labrum in a retrograde fashion by pulling the shuttling suture back out the anterior portal. Alternatively, to use a single anterior cannula for suture shuttling, the curved suture-passing gadget is passed beneath the labrum and the shuttling suture is superior so that an plentiful quantity of suture is collected throughout the joint. Next, the curved suture passer handle is removed rigorously from the anterior cannula with out removing the shuttling suture from beneath the labrum. Both limbs of the suture at the second are retrieved and parked out of the anterior cannula.
Syndromes
- Herpes infections
- Urination problems (too much or too little urine)
- Uncontrolled blood glucose in diabetics
- Genetic defects that affect the tooth enamel, such as dentinogenesis and amelogenesis
- Poor diet and nutrition, causing too little iron, folate, vitamin B12, or vitamin B6
- Hypervolemic hyponatremia -- both sodium and water content in the body increase, but the water gain is greater
- Time it was swallowed
Order asendin american express
The axons of the second neurons cross the m idline and journey in the trigem inothalam ic tract to the ventral posterom edial nucleus and to the intralam inar thalam ic nuclei on the opposite side, the place they term inate. The third (thalam ic) neuron of the ache pathway ends in the prim ary som atosensory cortex. In the trigem inal nerve it self, the other sensory bers run parallel to the ache bers but time period inate in various trigem inal nuclei (see p. Functiona l Systems Prefrontal cortex Thalam us Hypothalam us Amygdala Central gray (periaqueductal gray) m at ter Mesencephalon Anterior pretectal nucleus Locus coeruleus Raphe nuclei Descending noradrenergic and serotoninergic fibers B Pathw ays of the central descending analgesic system (after Lorke) Besides the ascending pathways that carry pain sensation to the first somatosensory cortex, there are also descending pathways which have the abilit y to suppress ache impulses. The central relay station for the descending analgesic (pain-relieving) system is the central grey (periaqueductal gray) m at ter of the mesencephalon. It is activated by a erent input from the hypothalam us, the prefrontal cortex, and the amygdaloid our bodies (part of the lim bic system, not shown). The axons from the excitatory glutam inergic neurons (red) of the central grey mat ter time period inate on serotoninergic neurons within the raphe nuclei and on noradrenergic neurons within the locus ceruleus (both proven in blue). They term inate instantly or indirectly (via inhibitory neurons) on the analgesic projection neurons (second a erent neuron of the pain pathway), thereby inhibiting the additional conduction of ache impulses. Posterolateral funiculus Processing and conduction of nociceptive signals within the spinal wire Nociceptive signal conduction in the peripheral nerve Processing of nociceptive indicators in the brain Pain notion General anesthesia, psychotherapeutic strategies System ic or epidural opiates, stim ulation therapy, neurosurgery Peripheral or epidural nerven block Inflam m ation, edem a, type ation of pain m ediators Tissue harm Im m obilization, cooling, analgesic m edication, anti-inflam m atory m edication C Pain perception and therapeutic interventions Peripheral ache m ay be attributable to native tissue harm from a bee sting, for examination ple. The inform ation on this injury is transm it ted by a quantity of relay stations to the prim ary som atosensory cortex, where the signals are perceived as ache (translated from easy encoded impulses). The cerebellar hem ispheres and basal ganglia work in parallel to program the m ovem ent and inform the prem otor cortex of the outcomes of this planning. The prem otor cortex passes the inform ation to the prim ary m otor cortex (M1), which relays the inform ation by way of the pyramidal tract to the alpha m otor neuron (pyramidal motor system). The alpha m otor neuron then transm it s the inform ation to the skeletal m uscle, which transform s the program into a specic voluntary m ovem ent. Sensorim otor functions provide necessary suggestions throughout this process (How far has the m ovem ent progressed Although som e of the later gures painting the prim ary m otor cortex as the begin line for a voluntary m ovem ent, this diagram reveals that m any m otor facilities are concerned within the execution of a voluntary m ovem ent (including the extrapyramidal motor system, see C and D; cerebellum). For sensible causes, nevertheless, the dialogue com m only begins at the prim ary m otor cortex (M1). Association cortex Planning Cerebellar hem ispheres Basal ganglia Premotor cortex Programming M1 Execution Cerebellar interm ediary Pyram idal tract Feedback B Cortical areas with motor operate: initiating a motion Lateral view of the left hemisphere. The initiation of a voluntary movement (reaching for a co ee cup) outcomes from the interaction of assorted cortical areas. The primary motor cortex (M1, Brodmann space 4) is located in the precentral gyrus (execution of a movement). The rostrally adjoining space 6 consists of the lateral premotor cortex and medial supplementary motor cortex (initiation of a movement). These areas present the cortical illustration of area, which is important in precision greedy actions and eye movements. Som atosensory inform ation Control Supplem entary m otor cortex Precentral gyrus (prim ary m otor cortex, M1) Prem otor cortex Prefrontal cortex Central sulcus Postcentral gyrus (prim ary som atosensory cortex) Posterior parietal cortex 444 Neuroa na tomy 20. Functiona l Systems Efferent fibers Motor thalam us Brainstem Pontine nuclei Corpus striatum Cortex Pallidum Basal ganglia Nuclei Cerebellum Tegm entum Red nucleus C Connections of the cortex with the basal ganglia and cerebellum: prog ramming of complex actions the pyram idal m otor system (the prim ary m otor cortex and the pyram idal tract arising from it) is assisted by the basal ganglia and cerebellum in the planning and program m ing of com plex m ovem ents. While a erent bers of the m otor nuclei (green) project directly to the basal ganglia (left) with out synapsing, the cerebellum is indirectly controlled through pontine nuclei (right; see C, p. The e erent bers of the basal nuclei and cerebellum are distributed to lower structures together with the spinal wire. The importance of the basal ganglia and cerebellum in voluntary m ovem ents can be appreciated by noting the e ects of lesions in these structures. While ailments of the basal ganglia impair the initiation and execution of m ovem ent s. Spinal twine Cerebral cortex Thalamus Basal ganglia Cerebellum Brainstem Spinal twine Motor inform ation Skeletal m otor function D Simpli ed block diagram of the sensorimotor system in the control of movement Voluntary m ovem ent s require constant suggestions from the periphery (m uscle spindles, tendon organs) in order to rem ain inside the desired lim it s. The spinal wire, brainstem, cerebellum, and cerebral cortex are the three control ranges of the sensorim otor system. All inform ation from periphery, cerebellum, and the basal ganglia passes by way of the thalam us on its method to the cerebral cortex. The medical importance of the sensory system in m ovem ent is illustrated by the sensory ataxia that m ay happen when sensory function is misplaced (see D, p.
Buy genuine asendin
Chemical messengers involved in local communication between cells are often identified as paracrine substances (or agents). With the exception of autocrine messengers, all messengers act between cells-that is, intercellularly. Homeostasis: A Framework for Human Physiology 11 by cells and launched, once given the appropriate stimulus, into the extracellular fluid. Rather, the chemical is secreted by a cell into the extracellular fluid and then acts upon the very cell that secreted it. Frequently, a messenger may serve both paracrine and autocrine features simultaneously-that is, molecules of the messenger launched by a cell could act domestically on adjacent cells as properly as on the identical cell that released the messenger. A neuron, endocrine gland cell, and other cell kind may all secrete the identical chemical messenger. In some circumstances, a selected messenger might typically function as a neurotransmitter, a hormone, or a paracrine or autocrine substance. All types of intercellular communication described up to now on this part involve secretion of a chemical messenger into the extracellular fluid. The first kind occurs via hole junctions, that are bodily linkages connecting the cytosol between two cells (see Chapter 3). Molecules can move immediately from one cell to an adjacent cell via hole junctions with out coming into the extracellular fluid. For instance, the messenger could additionally be a plasma membrane protein with part of its structure extending into the extracellular house. When the cell encounters one other cell sort capable of responding to the message, the 2 cells link up through the membrane-bound protein. This sort of signaling, typically termed juxtacrine, is of particular importance in the progress and differentiation of tissues in addition to in the functioning of cells that defend the body towards pathogens (Chapter 18). It is one way during which comparable types of cells "acknowledge" one another and type tissues. Let us take sweating in response to warmth exposure as an example and perform a simple experiment. On day 1, we expose an individual for half-hour (min) to an elevated temperature and ask her to do a standardized train test. The sweating offers a mechanism for rising warmth loss from the physique and due to this fact tends to minimize the increase in body temperature in a sizzling environment. Then, for per week, our subject enters the heat chamber for 1 or 2 hours (h) per day and workouts. On day eight, her body temperature and sweating rate are again measured during the same train take a look at performed on day 1. The hanging discovering is that the subject begins to sweat sooner and rather more profusely than she did on day 1. She has undergone an adaptive change induced by repeated publicity to the warmth and is now better capable of reply to heat publicity. The precise anatomical and physiological adjustments that bring about elevated capacity to withstand change during acclimatization are highly diversified. Typically, they involve an increase within the quantity, measurement, or sensitivity of one or more of the cell types in the homeostatic management system that mediates the fundamental response. Biological Rhythms As noted earlier, a striking attribute of many physique functions is the rhythmic modifications they manifest. The most common sort is the circadian rhythm, which cycles approximately as quickly as every 24 h. They add an anticipatory component to homeostatic control techniques, in impact, a feedforward system working without detectors. The unfavorable suggestions homeostatic responses we described earlier Body temperature (�C) 38 Lights on Lights off 37 36 6:00 A. Note the rise in physique temperature that happens simply prior to lights on, in anticipation of the increased exercise and metabolism that occur throughout waking hours.
Purchase asendin
The sensory ganglia contain the bodies of the pseudounipolar or bipolar (in case of the vestibulocochlear n. It s bers pass by way of the superior ganglion and finish within the spinal nucleus of the trigem inal n. Note: the cerebral cortex is the beginning and ending point for t wo loops, the basal-ganglia loop and the cerebellar loop. It picks up alerts from the basal ganglia and the cerebellum and relays the integrated impulse pat tern to the m otor cortex. At the sam e tim e, the thalam us receives enter from the sensory organs ("sensory thalam us"). If these alerts are related for m ovem ent, the thalam us feeds them into the impulse pat tern as above. Thus, the thalam us is the m ajor integration center for each loops as nicely as for sensory enter. The thalam ic im pulses eventually generate a "complete" detailed m ovem ent program. It is relayed to brainstem centers (red nucleus, reticular kind ation, inferior olivary nucleus) for ne tuning. The inferior olivary nucleus represents a particularly signi cant connection of the cerebellar loop towards the spinal twine. The m ovem ent is ultim ately initiated by im pulses from the m otor cortex (m ostly precentral gyrus), which attain the spinal wire by way of the pyram idal tract (here corticospinal tract) (for voluntary m ovem ent). The spinal wire it self executes the m ovem ent and sends the impulse by way of the spinal nerves to the corresponding m uscles. Inform ation in regards to the execution of m ovem ent is shipped through spinocerebellar tract s from the spinal cord to the cerebellum, which makes use of this inform ation for constantly m aking postural adjustm ents to have the ability to m aintain steadiness. The inferior olivary nucleus of the brainstem plays a signi cant role (c): It projects each to the cerebellum and to the spinal cord and receives a erent s from each regions. Additionally, the inferior olive receives a erents from different brainstem nuclei (red nucleus and reticular kind ation). All a erents end in the cortex with collaterals ending in cerebellar nuclei (not proven here). Histologically, the olivocerebellar tract is the one one that provides clim bing bers (they instantly finish on the Purkinje cells within the cortex). All different a erent s finish as m ossy bers on the granule cells in the cerebellar cortex. The cerebellar e erent s largely originate from the nuclei (see left aspect, b) and run either to the thala- m us (feedback loop to the telencephalon (see left aspect, a) or to brainstem nu-clei, which in flip project to the spinal cord through extrapyram idal tracts and thus control m otor features (cf. The projection from the vestibular nuclei to the nuclei that control eye m ovem ents help with com pensatory eye m ovem ent s throughout head m ovem ent. Note: A direct projection of the cerebellum to the spinal twine has not been so far confirmed in hum ans. There, association pathways connect di erent cortical areas of the sam e hem isphere (they by no means cross). There are three distinct t ype of affiliation bers: � Arcuate bers (not proven here) join adjcent gyri. Note: the bers of the vertical occipital fasciculi join lateral temporal and parietal lobes and cross the occipital lobe. Motor im pulses from the cerebral cortex thus journey to contralateral subcortical centers and in uence m otor activit y of the contralateral aspect of the physique. Y the thalam us itself, is reached by pathways of subordinate et, facilities, m ost of that are positioned contralaterally. Subsequently, sensory impulses to the cerebral cortex originate m ainly from the contralateral aspect of the body. Exceptions to this basic precept: � Motor function: cortical projections to individual m otor nuclei of cranial nerves (see p. Neuron Superior olivary nucleus Right Lateral lem niscus Red nucleus Cerebellum Pallidum c Inferior olivary nucleus Pyram id (with corticospinal fibers) Rubroolivary tract Olivocerebellar tract Cerebelloolivary fibers Thalam us Inferior olivary nucleus Spinoolivary fibers Olivospinal tract Anuloolivary fibers 2. Neuron Posterior cochlear nucleus Spinal twine A De nition of the terms "olive," "inferior," and "superior olive" and connections of each olives a Brainstem, ventral view; b Cross-section of the m edulla oblongata close to the pons- superior view; c Cross-section of m edulla oblongata- inferior view. It is located contained in the m edulla oblongata, mediodorsal and largely cranial to the inferior olive and is thus clearly seen on cross-sections directly caudal to the pons (b). Due to the partial overlap of the inferior and superior olive, both nuclear complexes are sometim es seen on sam e cross-sections.
Asendin 50mg discount
Neurological deficit, top loss of greater than 50%, and kyphosis higher than 20� are predictors of instability which require surgical intervention. Absolute indications for surgical intervention in thoracolumbar burst fractures are progressive neurological deficit, cauda equina syndrome, and vital spinal instability regardless of bracing. Neurologic restoration from thoracolumbar burst fractures: Is it predicted by the amount of initial canal encroachment and kyphotic deformity Relationship between traumatic spinal canal stenosis and neurologic deficits in thoracolumbar burst fractures. Operative in contrast with nonoperative remedy of a thoracolumbar burst fracture with out neurological deficit: A potential, randomized study. It attaches to the medial features of the lateral plenty of C1 and prevents posterior displacement of the C2 odontoid peg relative to the anterior arch of C1. Biomechanical research have discovered that after a mixed lateral displacement of 7 mm or more occurs there might be additional lateral displacement regardless of immobilization as the transverse ligament has ruptured. These unstable injuries cause long-term quality-of-life problems for patients, especially these with vital displacement or associated injuries. Unilateral C1 lateral mass sagittal cut up fracture: an unstable Jefferson fracture variant. Anterior retropharyngeal fixation C1/2 for stabilisation of atlantoaxial instabilities: Study of feasibility, technical description and preliminary outcomes. Spiral computed tomography for the prognosis of cervical, thoracic and lumbar backbone fractures: its time has come. Computed tomography versus plain radiography to display screen for cervical backbone harm: a meta-analysis. The axis of rotation with this mechanism of damage is anterior to the vertebral body. In explicit, the posterior ligamentous complex may be disrupted allowing dislocation of the aspects with instability and the danger of great neurological harm. Surgical end result of thoracolumbar burst fractures with flexion�distraction damage of the posterior elements. Previous theories had advised that decompressing the cervical spine could be including an additional secondary harm to the spinal twine. Methylprednisolone or naloxone remedy after acute spinal cord harm: 1 yr follow up information. The urgency of surgical decompression in acute central cord injuries with spondylosis and without instability. Neurological outcome of early versus late surgical procedure for cervical spinal twine damage. Reduction in Gardner�Wells tongs with serial traction Surgical open discount could increase the neurological deficit if a disc herniation exists. Evidence from animal research means that speedy decompression of the spinal twine may improve restoration. Pathophysiology of spinal twine damage: restoration after quick and delayed decompression. Extrusion of an intervertebral disc related to traumatic subluxation or dislocation of cervical sides: case report. Should this happen, then other options must be discussed with the patient, together with occipitocervical fusion. Thoracolumbar flexion-distraction accidents: associated morbidity and neurological outcomes. Which of the following options is associated with humeral head ischaemia after a proximal humerus fracture A 60-year-old woman slips, sustaining a comminuted intra-articular distal humeral fracture. Open discount internal fixation with plating and a lag screw via the plate D. Which of the following is the most acceptable management for the radial head component of this injury Open discount and inside fixation with buried compression screws � a low-profile plate onto the radial neck within the protected zone B. Radial head arthroplasty utilizing a modular steel press-fit design with care to not over-stuff the joint.